

Vitorino Modesto dos Santos1; Taciana Arruda Modesto Sugai3; Fabiano Girade Corrêa1; Elber Rocha Barbosa Júnior1; Fluvia Manuela Canhete Siqueira1; Antônio Victor Paes de Vasconcelos2
DOI: 10.1590/S0004-27492007000100033
ABSTRACT
Alcohol-related massive eyelid edema has been rarely reported. The differential diagnosis includes local and systemic conditions. Alcohol itself can be associated with dermatological hypersensitivity reactions, appearing soon after alcoholic drinks. Massive bilateral eyelid swelling can constitute diagnostic pitfalls and therapeutic challenges to general practitioners with a placebo.
Keywords: Alcoholism; Edema; Eyelids; Lymphedema; Case reports
RESUMO
Edema palpebral maciço relacionado ao uso de álcool tem sido raramente descrito. O diagnóstico diferencial inclui condições locais e sistêmicas. O próprio álcool pode estar associado com reações dermatológicas de hipersensibilidade, surgindo logo após uso de bebidas alcoólicas. Edema palpebral bilateral maciço pode constituir embaraços diagnósticos e desafios terapêuticos para os clínicos.
Descritores: Alcoolismo; Edema; Pálpebras; Linfedema; Relatos de casos
RELATOS DE CASOS
Alcohol-related massive eyelid swelling: case report
Edema palpebral maciço relacionado ao uso de álcool: relato de caso
Vitorino Modesto dos SantosI; Taciana Arruda Modesto SugaiII; Fabiano Girade CorrêaIII; Elber Rocha Barbosa JúniorIII; Fluvia Manuela Canhete SiqueiraIII; Antônio Victor Paes de VasconcelosIV
IMD, PhD, Department of Internal Medicine from Armed Forces Hospital - HFA - Brasília (DF) - Brazil; Catholic University Medical Course - Brasília (DF) - Brazil
IIMD, Specialist from the Brazilian Society of Dermatology - Brasília (DF) - Brazil
IIIMD, Department of Internal Medicine from HFA - Brasília (DF) - Brazil
IVMedical Student, Catholic University Medical Course - Brasília (DF) - Brazil
ABSTRACT
Alcohol-related massive eyelid edema has been rarely reported. The differential diagnosis includes local and systemic conditions. Alcohol itself can be associated with dermatological hypersensitivity reactions, appearing soon after alcoholic drinks. Massive bilateral eyelid swelling can constitute diagnostic pitfalls and therapeutic challenges to general practitioners with a placebo.
Keywords: Alcoholism/complications; Edema; Eyelids; Lymphedema; Case reports [publication type]
RESUMO
Edema palpebral maciço relacionado ao uso de álcool tem sido raramente descrito. O diagnóstico diferencial inclui condições locais e sistêmicas. O próprio álcool pode estar associado com reações dermatológicas de hipersensibilidade, surgindo logo após uso de bebidas alcoólicas. Edema palpebral bilateral maciço pode constituir embaraços diagnósticos e desafios terapêuticos para os clínicos.
Descritores: Alcoolismo/complicações; Edema; Pálpebras; Linfedema; Relatos de casos [tipo de publicação]
INTRODUCTION
Massive swelling of the eyelids is a rare condition that can cause severe visual impairment and has been associated with rosaceous lymphedema(1-2).
Causes of orofacial edema includes: angioedema; Ascher's syndrome; scleredema adultorum of Buschke; cardiac, endocrine, hepatic and renal disease; Crohn's disease; drugs; infections; kwashiorkor; lymphatic stasis; Melkersson-Rosenthal syndrome; morbus morbihan; neoplasms; rosacea; sarcoidosis; storage disease; urticaria; and vena cava obstruction(1-8).
About 90% of chronic alcoholics may show skin, hair, nail or oral changes, some associated with malnutrition, poor hygiene, and smoking. The following skin changes are common after a decade of heavy drinking: clubbing; eczema; erythema; flushing; gingivitis; glossitis; icterus; infections; koilonychias; leukoplakia; lichenoid dermatitis; pellagra; porphyria; pruritus; psoriasis; purpura; rosacea; seborrheic dermatitis; telangiectasis; and tinea versicolor(9).
Alcohol consumption constitutes a long-term relentless problem of public health in the whole world; nevertheless, ethanol abuse has not been pursued as it should be(10). Moreover, among women and old-aged men, the characterization of alcohol-related conditions is often more difficult than among young males(11).
CASE REPORT
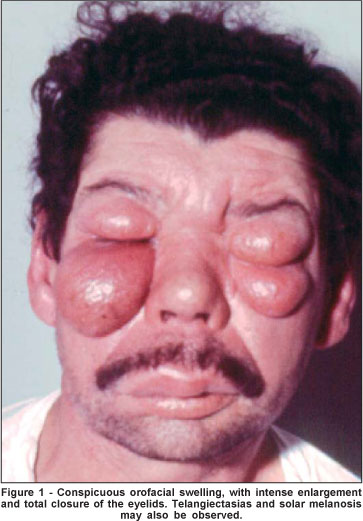
A 43-year-old Brazilian nonatopic male came to the hospital complaining of a disfiguring symmetrical eyelid swelling, with impaired vision. He denied drug use, but consumed alcohol (70-140 g/week) and tobacco for more than ten years. In the last 2 years, he presented episodic pruritic facial swelling, more evident on the eyelids, with an ethanol dose-response effect following the spirit drinking binges. There was no either personal or family history of allergy or antecedent of hypersensitivity diseases, and the patient was not using any medicine. On physical examination, the disfiguring edema was restricted to the face, and the eyelids were the most affected areas. The huge symmetrical enlargement impaired the vision due to closure of the eyes, and mid third of the face and the upper lip were also affected (Figure 1). The oral cavity, teeth and tongue showed no abnormalities. There was no evidence of parotiditis, rosaceous lymphedema, scleredema, or skin infection. The ophthalmologic examination resulted normal, except for the massive bilateral eyelid swelling of elastic consistency. The stigmata of cardiac, endocrine, hepatic, renal, or storage diseases were absent. The cranial nerves and the vital signs were normal. Laboratory tests showed high levels of gamma-glutamyltransferase, aminotransferases, and 420 IU/ml total IgE. The titers of antineutrophil cytoplasmic antibodies were normal. No abnormalities were found in the complement system. The skin-prick tests against aeroallergens, and the patch tests for contact hypersensitivity resulted negative. The blood count cells, the urinalysis, the levels of electrolytes, calcium, glucose, albumin, and prothrombin activity were all normal. The tests of renal and thyroid functions and the chest X-ray resulted normal. Positive results were found on screening for alcohol, but neither clinical findings nor laboratory parameters characterized liver cirrhosis. Without medication, after a watchful waiting period of two weeks following ethanol abstinence, the facial edema spontaneously regressed; further, total IgE serum level progressively decreased until reaching its normal limit. Skin sample from the right inferior eyelid showed no evidence of extracellular deposits, granulomas or lymphatic changes (Figure 2). The patient persisted without eyelid swelling, maintaining alcohol abstinence for more than two years.
DISCUSSION
By not entirely clear mechanisms, alcohol users present hypersensitivity reactions, as exercise-induced anaphylaxis, angioedema, asthma attacks, food allergies, urticaria and IgE-mediated reactions(9). Moreover, alcoholic liver disease can play a role in the genesis of allergic skin reactions(12); and alcohol intake has been associated with distinctive skin changes and exacerbation of dermatologic disorders(9,13).
This nonatopic chronic alcoholic patient presented severe disfiguring edema restricted to the orofacial region, and the episodes occurred, exclusively, soon after drinking binges. The differential diagnosis of chronic facial edema includes local and systemic conditions(3). In the present case, the findings favor the hypothesis of an ethanol-related orofacial edema, and hypersensitivity reaction after alcoholic drinks. A major concern was about the differential diagnosis with contact dermatitis, recurrent idiopathic angioedema(14), and the monosymptomatic presentation of the Melkersson-Rosenthal syndrome(7). These, and the other above mentioned conditions, were ruled out based on the clinical data, complete questionnaire, patch testing, and skin biopsy. Although one can hardly prove that alcohol was the sole stimulus in the present case; as a whole, the data strongly indicate the major role of ethanol in the genesis of the eyelid swelling. Moreover, after a long period of surveillance without medications, the patient remains in alcohol abstinence and entirely free of the repetitive episodes of orofacial edema.
CONCLUSIONS
Huge eyelid swelling with impaired vision may be related to alcohol ingestion. Alcohol intake is associated with exacerba- tions of existing dermatologic disorders. Alcoholism can be involved in angioedema, anaphylaxis, and IgE-mediated reactions.
Low socioeconomic status may enhance the severity of alcohol-related skin disorders.
Eyelid changes following chronic heavy drinking seem to be underreported.
Alcohol-related massive eyelid swelling can also constitute a diagnostic pitfall in clinical practice.
REFERENCES
1. Spallek G, Buttgereit F, Audring H, Hiepe F. Persistent facial swelling of unclear etiology. The differential diagnostic considerations. Hautarzt. 1997;48 (11):828-33. Id: Ger.
2. Marzano AV, Vezzoli P, Alessi E. Elephantoid edema of the eyelids. J Eur Acad Dermatol Venereol. 2004;18(4):459-62.
3. Bernardini FP, Kersten RC, Khouri LM, Moin M, Kulwin DR, Mutasim DF. Chronic eyelid lymphedema and acne rosacea. Report of two cases. Ophthalmology. 2000;107(12):2220-3.
4. Ioannidou DI, Krasagakis K, Stefanidou MP, Karampekios S, Panayiotidis J, Tosca AD. Scleredema adultorum of Buschke presenting as periorbital edema: a diagnostic challenge. J Am Acad Dermatol. 2005;52(2 Suppl 1):41-4.
5. Litvyakova LI, Bellanti JA. Orofacial edema: a diagnostic and therapeutic challenge for the clinician. Ann Allergy Asthma Immunol. 2000;84(2):188-92.
6. Lai TF, Leibovitch I, James C, Huilgol SC, Selva D. Rosacea lymphoedema of the eyelid. Acta Ophthalmol Scand. 2004;82(6):765-7.
7. Nossa LMB, Costa AL, Marback RL. Síndrome de Melkersson-Rosenthal: estudo clínico-patológico de um caso. Arq Bras Oftalmol. 2001;64(6):573-5.
8. Wohlrab J, Lueftl M, Marsch WC. Persistent erythema and edema of the midthird and upper aspect of the face (morbus morbihan): evidence of hidden immunologic contact urticaria and impaired lymphatic drainage. J Am Acad Dermatol. 2005;52(4):595-602.
9. Rao GS. Cutaneous changes in chronic alcoholics. Indian J Dermatol Venereol Leprol. 2004;70(2):79-81.
10. Rosa AA, Gonçalves SC, Stefani SD, Martins SO, Rosa DD, Hunsche A, et al. Percepção e registro de abuso de álcool e de doenças relacionadas num hospital geral universitário. Rev Assoc Med Bras (1992). 1998;44(4):335-9.
11. Booth BM, Blow FC, Cook CA, Bunn JY, Fortney JC. Age and ethnicity among hospitalized alcoholics: a nationwide study. Alcohol Clin Exp Res. 1992;16(6):1029-34.
12. Mujagic H, Prnjavorac B, Mujagic Z, Festa G. Alcohol in alcoholic liver disease is a causative factor for development of allergic skin manifestations. Med Arh. 2003;57(5-6):273-8.
13. Muller BA. Urticaria and angioedema: a practical approach. Am Fam Physician. 2004;69(5):1123-8. Review.
14. Smith KE, Fenske NA. Cutaneous manifestations of alcohol abuse. J Am Acad Dermatol. 2000;43(1 Pt 1):1-16; quiz 16-8.
 Address to correspondence:
Address to correspondence:
Vitorino Modesto dos Santos
SMPW - Quadra 14 - Conjunto 2 - Lote 7 - Casa A - Brasília (DF)
CEP 71745-140
E-mail: [email protected]
Recebido para publicação em 26.01.2006
Última versão recebida em 13.03.2006
Aprovação em 22.05.2006
Competing interests: The authors have no conflict of interest to disclose
Nota Editorial: Depois de concluída a análise do artigo sob sigilo editorial e com a anuência do Dr. Sérgio Felberg sobre a divulgação de seu nome como revisor, agradecemos sua participação neste processo.
© 2024 - All rights reserved - Conselho Brasileiro de Oftalmologia
![]()
 English PDF
English PDF
 Print
Print
 Send this article by email
Send this article by email
 How to cite this article
How to cite this article
 Submit a comment
Submit a comment
 Mendeley
Mendeley
 Scielo
Scielo
 Pocket
Pocket
