Arq. Bras. Oftalmol. 2025;88 (6 )
:1-8
| DOI: 10.5935/0004-2749.2025-0077
Abstract
PURPOSE: Standard intravitreal medication dosages are based on an assumed vitreous cavity volume of 4.0-4.5 mL. However, individual variations in vitreous cavity volume may influence both the efficacy and safety of these medications. This study proposes dosage adjustments for intravitreal medications and gases according to axial length and the corresponding vitreous cavity volume.
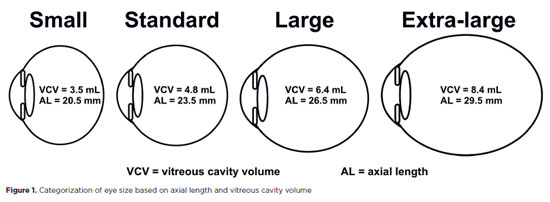
METHODS: This descriptive study employed reference guidelines that use axial length to estimate the Axial Length-based Volume of the Vitrectomized Space and the Vitreous Volume EXact table for determining dose adjustments across varying eye sizes. Small eyes (axial length 19-22 mm) have an average vitreous cavity volume of 3.5 mL at an axial length of 20.5 mm; standard-sized eyes (22-25 mm) have 4.8 mL at 23.5 mm; large eyes (25-28 mm) have 6.4 mL at 26.5 mm; and extra-large eyes (28-32 mm) have 8.4 mL at 29.5 mm. The medications considered included anti-infectives, anti-VEGFs, complement inhibitors, recombinant proteases, chemotherapy agents, corticosteroids, and medical gases.
RESULTS: Analysis of intravitreal drug concentrations relative to vitreous cavity volume demonstrated notable variability when a standard dose was administered. Small eyes received about 135% of the concentration intended for a standard-sized eye; large eyes received around 75%; and extra-large eyes received under 60%. The recommended dose adjustments are as follows: for small eyes, administer 70-80% of the standard dose; for large eyes, 130-140%; and for extra-large eyes, 170-180%.
CONCLUSIONS: Tailoring intravitreal drug and gas dosages according to axial length and vitreous cavity volume may enhance intraocular drug distribution, potentially improving both safety and therapeutic outcomes.
Keywords: Intravitreal injections; Axial length; Vitreous body; Drug dosage calculations; Pharmacokinetics; Anti-infective agents
Arq. Bras. Oftalmol. 2025;88 (4 )
:1-7
| DOI: 10.5935/0004-2749.2024-0229
Abstract
PURPOSE: The volume of the vitreous chamber varies with the size of the eye. The space created in the vitreous cavity by a vitrectomy is called the vitrectomized space. The volume of the vitrectomized space is strongly correlated with the axial length of the eye. This study aims to present guidelines for estimating the using participants stratified by axial length, sex, and history of cataract surgery.
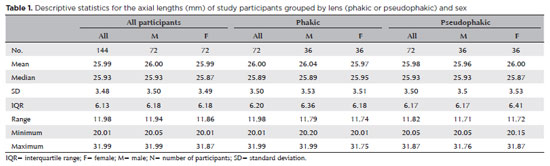
METHODS: This retrospective, observational, cross-sectional study included 144 randomly selected participants who underwent vitrectomies between 2013 and 2023. Before surgery, the axial lengths of participants' eyes were measured using optical biometrics. The axial lengths of the eyes in our sample were between 20-32 mm. In all cases, a complete vitrectomy was performed, followed by complete fluid-air exchange and injection of a balanced saline solution. The volume infused was recorded.
RESULTS: The median (interquartile range; range) volume of the vitrectomized space was 6.1 (3.8; 3.1-11.3) mL in men and 6.1 (3.3; 3.2-11.2) mL in women (p=0.811). The median volume of the vitrectomized space was 5.9 (3.6; 3.1-11.2) mL in patients with phakic lenses and 6.25 (3.6; 3.3-11.3) mL in those with pseudophakic lenses (p=0.533). A positive correlation was found between the axial length and the volume of the vitrectomized space in this sample (r=0.968; p<0.001). In a cubic polynomial regression, the coefficient of determination was 0.948. Similar results were observed in both sexes and in both phakic and pseudophakic patients. The estimated cubic polynomial regression equation for this sample was VVS = 0.000589052857847605 × AL3 - 0.025114926401582700 × AL2 + 0.685961117595624000 × AL - 5.088226672620790000.
CONCLUSION: We developed this axial length estimation of the volume of vitrectomized space as a guideline for the determination of vitrectomized space volume using axial length.
Keywords: Cataract extraction; Retinal perforations/surgery; Epiretinal membrane/surgery; Vitreous body; Axial length, eye; Vitrectomy; Biometry/methods; Diagnostic techniques, ophthalmological; Guidelines as topic.
Arq. Bras. Oftalmol. 2026;89 (3 )
:1-7
| DOI: 10.5935/0004-2749.2025-0392
Abstract
PURPOSE: To evaluate the accuracy of a short-term intravitreal dexamethasone sodium phosphate challenge in predicting the anatomical response to a sustained-release dexamethasone implant (Ozurdex) in patients with refractory diabetic macular edema.
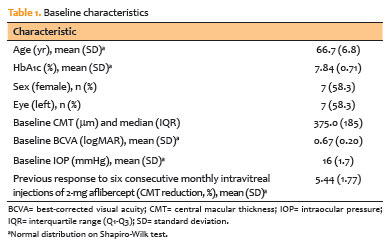
METHODS: This prospective, non-randomized, Phase 2 pilot study enrolled 12 pseudophakic eyes with diabetic macular edema refractory to anti-vascular endothelial growth factor (anti-VEGF) therapy. Participants underwent a challenge phase (Day 0) consisting of a single intravitreal injection of 0.08-mg dexamethasone sodium phosphate, followed by a maintenance phase (Day 7), during which all subjects received a 0.7-mg dexamethasone implant. The primary outcome was concordance between the anatomical response at Day 3 (post-dexamethasone sodium phosphate) and Day 60 (post-implant), defined as a ≥10% reduction in central macular thickness. Secondary outcomes included achieving a clinically "dry" macula (central macular thickness ≤300 μm) at Day 60, changes in best-corrected visual acuity, safety outcomes (intraocular pressure), and spectral-domain optical coherence tomography biomarker analysis.
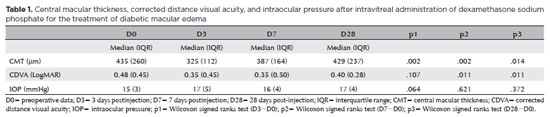
RESULTS: The dexamethasone sodium phosphate challenge induced significant macular drying by Day 3 (median central macular thickness reduction, −21 μm; p=0.002). A positive response to dexamethasone sodium phosphate strongly predicted response to the dexamethasone implant, with a positive predictive value and specificity of 100%. The negative predictive
value was 80%. Irreversible biomarkers, including disorganization of retinal inner layers and ellipsoid zone disruption, were more prevalent among nonresponders (60% vs. 28.6%). Safety outcomes were acceptable; 16.7% of patients developed ocular hypertension, which was successfully managed with topical therapy.
CONCLUSION: A short-term dexamethasone sodium phosphate challenge is a safe,
low-cost, and highly specific predictor of dexamethasone implant efficacy. This "test-and-treat" strategy may optimize resource allocation in resource-constrained settings by identifying responders before high-cost implantation.
Keywords: Diabetic retinopathy; Macular edema; Dexamethasone; Drug implants; Biomarkers, pharmacological
Arq. Bras. Oftalmol. 2025;88 (5 )
:1-8
| DOI: 10.5935/0004-2749.2024-0098
Abstract
PURPOSE: To compare the short-term (3-month) outcomes of intravitreal aflibercept injections versus intravitreal aflibercept combined with dexamethasone sodium phosphate in treating diabetic macular edema.
METHODS: In this Phase-2 clinical trial, 16 eyes of 16 participants with diabetic macular edema were randomly assigned to one of 2 groups. Participants in the aflibercept monotherapy group received 2 mg of intravitreal aflibercept (0.05 mL), while those in the combination therapy group received 2 mg of intravitreal aflibercept (0.05 mL) plus 0.04 mg dexamethasone sodium phosphate (0.01 mL). Identical injections were repeated after 30 and 60 days. The primary outcome was the change in central macular thickness, as measured by optical coherence tomography, from baseline to 1 month after the last injection. Secondary outcomes included changes in best-corrected visual acuity and intraocular pressure over the same period.
RESULTS: The mean baseline central macular thickness was 444 ± 86 μm in the combination therapy group and 394 ± 96 μm in the aflibercept monotherapy group (p=0.293). By day 90, the mean reduction in central macular thickness was significantly greater in the combination therapy group (176 ± 129 μm) compared to the aflibercept monotherapy group (54 ± 49 μm; p=0.034). Best-corrected visual acuity also improved significantly more in the combination therapy group, with a median gain of 0.31 ± 0.16 LogMAR, whereas the aflibercept monotherapy group experienced a minimal change (−0.06 ± 0.13 LogMAR; p=0.020). Intraocular pressure remained stable in both groups, with no significant difference (p=0.855). None of the participants developed elevated intraocular pressure (>21 mmHg) or required ocular hypotensive medications. No significant ocular or systemic adverse events were reported.
CONCLUSION: The addition of dexamethasone sodium phosphate to the standard intravitreal aflibercept regimen for diabetic macular edema can improve short-term structural and functional outcomes.
Trial registration: Brazilian Clinical Trials Registry (RBR-7468j4q)
Keywords: Diabetic macular edema; Aflibercept; Dexamethasone sodium phosphate; Intravitreal injection; Visual acuity; Central macular thickness; Intraocular pressure
 ABO is licensed under a Creative Commons Attribution-NonComercial 4.0 Internacional.
ABO is licensed under a Creative Commons Attribution-NonComercial 4.0 Internacional.