Arq. Bras. Oftalmol. 2025;88 (6 )
:1-5
| DOI: 10.5935/0004-2749.2024-0340
Abstract
PURPOSE: This study aimed to report the surgical outcomes and success predictors of micropulse transscleral cyclophotocoagulation in eyes with refractory glaucoma.
METHODS: This was a noncomparative, interventional case series. Patients with refractory glaucomas, defined as eyes with prior incisional glaucoma surgery failure and uncontrolled intraocular pressure, who underwent micropulse transscleral cyclophotocoagulation between March 2017 and June 2021 were enrolled. A minimum follow-up period of 6 months was required. Preoperative and postoperative intraocular pressure, number of hypotensive medications, surgical complications, and any subsequent related events were recorded. Success criteria were as follows: 1) intraocular pressure reduction ≥20% and intraocular pressure ≤18 mmHg; 2) intraocular pressure reduction ≥30% and intraocular pressure ≤15 mmHg. The need for topical hypotensive medications was not considered a failure.
RESULTS: Seventy-nine (79) eyes (79 patients; mean age, 57.5 ± 20.6 years) were included. Overall, the median follow-up duration was 12.0 (interquartile interval, 6–24) months, and the mean intraocular pressure was reduced from 22.8 ± 6.8 mmHg to 15.5 ± 5.6 mmHg at the last follow-up visit (p<0.001). The mean number of medications was reduced from 2.8 ± 0.7 to 2.0 ± 1.0 (p<0.01). At 12 months postoperatively, the success rates for criteria 1 and 2 were 54.9% and 49.7%, respectively. Aside from one case of corneal ulcer, which fully resolved with clinical treatment, and two cases of persistent hypotony (with no visual acuity loss during follow-up), no other vision-threatening complications were observed during the postoperative period. The magnitude of intraocular pressure reduction at 1 month (adjusted to preoperative intraocular pressure; HR=1.01; p=0.002).
CONCLUSION: Our findings suggest that micropulse transscleral cyclophotocoagulation is a relatively effective alternative for managing refractory glaucomas, with minor postoperative complications. In addition, the initial intraocular pressure reduction was a statistically significant predictor of 1-year success in patients undergoing micropulse transscleral cyclophotocoagulation.
Keywords: Intraocular pressure/physiology; Glaucoma, open-angle/surgery; Trabeculectomy; Laser coagulation/methods; Tonometry, ocular/methods; Postoperative complications; Antihypertensive agents/therapeutic use.
Arq. Bras. Oftalmol. 2025;88 (3 )
:1-7
| DOI: 10.5935/0004-2749.2023-0309
Abstract
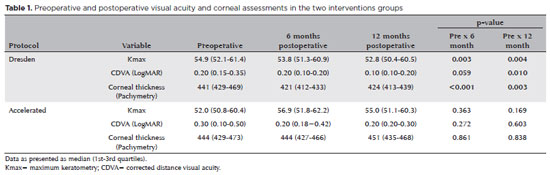
PURPOSE: Keratoconus presents certain peculiarities in pediatric patients when compared with adults. The greatest challenge in children is that the disease is more severe and faster in progression. In this retrospective study, we aimed to compare the accelerated and Dresden protocols for corneal crosslinking in patients aged <18 years who were followed-up for at least 12 months.
METHODS: A total of 36 eyes from 27 patients were included in the study. The best corrected and uncorrected visual acuity, maximal keratometry, corneal thickness, foveal thickness, and endothelial microscopy findings were evaluated at baseline and during the postoperative period at one, three, and six months. Thereafter, the patients were evaluated at one, three, six and twelve months postoperative. Corneal crosslinking was performed in all patients via the Dresden protocol (n=21 eyes) or the accelerated protocol (n=15 eyes). Data between the two groups were compared and XY statistical analysis was used.
RESULTS: Both protocols were effective in halting keratoconus progression. No patient had progression at the 12-month follow-up. A significant reduction in Kmax and improvement in the corrected distance visual acuity were observed only in the Dresden protocol group. Although the Dresden protocol was superior to the accelerated protocol in reducing Kmax (p=0.002), there was no significant difference in corrected distance visual acuity between the two groups.
CONCLUSION: The accelerated protocol is as efficient as the Dresden protocol in stabilizing keratoconus progression. Although the Dresden protocol was superior to the accelerated protocol in reducing the Kmax, it did not produce better clinical results. Thus, the accelerated protocol is an efficient option. Furthermore, considering the advantages of reduced surgical time, the accelerated protocol is effective in halting keratoconus progression in the pediatric age group.
Keywords: Keratoconus; Corneal diseases; Ultraviolet rays; Cross-linking reagents; Visual acuity
Arq. Bras. Oftalmol. 2025;88 (5 )
:1-7
| DOI: 10.5935/0004-2749.2024-0217
Abstract
PURPOSE: This study aimed to evaluate the influence of intrastromal corneal ring segment implants on the intraocular pressure measurements using Goldmann applanation tonometry, rebound tonometry, and noncontact tonometry in keratoconic corneas and analyze the intertonometer agreement.
METHODS: We enrolled 74 eyes in this observational and prospective study. Each participant had a complete eye examination, corneal analysis with Scheimpflug Tomography (Pentacam®), and intraocular pressure evaluation with Goldmann applanation tonometry, rebound tonometry, and noncontact tonometry, before and after intrastromal corneal ring segment implantation (on postoperative days 1, 7, 45, and 90). Intertonometer agreement was assessed using Bland-Altman analysis.
RESULTS: The mean age was 29.9 ± 10.2 years, and 47 (63.5%) eyes had keratoconus grade II. Intraocular pressures were higher for noncontact tonometry preoperatively and on 90 postoperative day (mean ± SD: 12.4 ± and 12.1 ± 2.2 mmHg, respectively), followed by Goldmann applanation tonometry (11.1 ± 3.0 and 11.2 ± 2.7 mmHg, respectively), and were lower for rebound tonometry (9.7 ± and 9.4 ± 3.2 mmHg, respectively). The variation from the Goldmann tonometry on 7 postoperative day to the baseline (p=0.022) and that of noncontact tonometry on 90 postoperative day to the baseline (p=0.021) were statistically significant. The rebound tonometry underestimated intraocular pressure when compared with the Goldmann applanation tonometry by a mean of 1.47 ± 5.19 mmHg. Noncontact tonometry, when compared with Goldmann applanation tonometry, overesti-mated intraocular pressure by a mean of 1.23 ± 4.15 mmHg.
CONCLUSION: Despite statistically significant differences between some postoperative periods, the intraocular pressure measurement differences may not be clinically relevant.
Keywords: Keratoconus; Intraocular pressure; Cornea; Corneal stroma; Postoperative period; Tonometry ocular; Prostheses and implants
 ABO is licensed under a Creative Commons Attribution-NonComercial 4.0 Internacional.
ABO is licensed under a Creative Commons Attribution-NonComercial 4.0 Internacional.