Arq. Bras. Oftalmol. 2026; 89 (3): 10.5935/0004-2749.2025-0263
Total: 462
Mahmut Oğuz Ulusoy; Muhammed Yelkovan; Ayna Sarıyeva-İsmayilov; Cansu Erseven
DOI: 10.5935/0004-2749.2025-0263
ABSTRACT
PURPOSE: To compare patients who underwent scleral fixation using the Yamane technique with and without simultaneous pars plana vitrectomy.
METHODS: A total of 37 patients were included in the study. Eighteen underwent simultaneous pars plana vitrectomy. The Yamane technique alone was performed only in patients with aphakia who had previously undergone pars plana vitrectomy for various reasons. Final lens position, best corrected visual acuity spherical equivalent, complication rates, and optical coherence tomography findings were recorded.
RESULTS: The duration of aphakia before intraocular lens implantation ranged from 1 month to 21 yr. Postoperative best corrected visual acuity improved in both groups, with no statistically significant difference (with pars plana vitrectomy: 0.42 ± 0.34; without pars plana vitrectomy: 0.32 ± 0.26; p=0.33). The spherical equivalent was also not significantly different between groups (with pars plana vitrectomy: 0.29 ± 1.08; without pars plana vitrectomy: 0.65 ± 2.23; p=0.53). There were no significant differences between the groups in complication rates, postoperative intraocular lens position or optical coherence tomography findings.
CONCLUSION: There was no difference in terms of safety or efficacy between the two approaches. Surgical decisions may be based on the surgeon’s experience and the patient’s systemic and ocular condition.
Keywords: Lens implantation, intraocular; Tomography, optical coherence; Vitrectomy; Intraocular lenses; Visual acuity; Aphakia; Yamane technique
INTRODUCTION
Several methods exist for correcting aphakia without sulcus support. The main distinction is between anterior and posterior approaches. Posterior scleral fixation of intraocular lenses is generally preferred over anterior fixation methods, such as iridocorneal angle-supported or iris-claw lenses(1). The Yamane technique is a novel sutureless scleral fixation method described by Shin Yamane in 2017(2). This technique has been widely adopted by ophthalmologists and is used in various types of aphakia, including traumatic and pediatric cases(3,4).
The most common causes of aphakia are cataract surgery and trauma. Management of these conditions often requires anterior or pars plana vitrectomy(5,6). Aphakia correction can be performed either simultaneously with vitrectomy or as a separate procedure. Simultaneous surgery may allow additional interventions and resolve the condition in a single step. However, in some cases, the ocular condition does not permit multiple procedures to be performed at the same time.
This study aimed to compare outcomes of the Yamane technique performed either simultaneously with or separately from pars plana vitrectomy.
METHODS
In this retrospective study, we compared data from patients who underwent Yamane scleral fixation either with simultaneous pars plana vitrectomy or as a separate procedure. All patients in the Yamane-only group had previously undergone pars plana vitrectomy for various reasons.
The study was conducted at the Department of Ophthalmology, Bursa Yüksek İhtisas Research Hospital, in accordance with the tenets of the Declaration of Helsinki. Approval was obtained from the Institutional Review Board and Ethics Committee (Project nº. 2011-KAEK-25-2023/12-07).
We compared data between the two groups, including best corrected visual acuity (BCVA) measured with the Snellen chart, intraocular pressure (IOP) (mmHg), spherical equivalent, follow-up duration, causes of aphakia, final intraocular lens position, OCT findings, and complications. Aphakia duration in the Yamane-only group was also recorded.
Exclusion criteria included patients with trauma, corneal opacities, retinal or vitreous abnormalities, glaucoma, optic nerve diseases, and systemic diseases that may affect the retina or optic nerve (e.g., diabetes mellitus). For the simultaneous PPV group, an additional exclusion criterion was concomitant retinal surgery (e.g., retinal detachment, epiretinal membrane, or macular hole).
Statistical analysis
Statistical analysis was performed using SPSS version 21.0 (SPSS, Chicago, Illinois). Data are presented as mean ± standard deviation. Normality was assessed using the Kolmogorov–Smirnov test. Student’s t test was applied based on normality results. A p-value <0.05 was considered statistically significant. Correlations between variables were evaluated using Pearson or Spearman correlation coefficients.
RESULTS
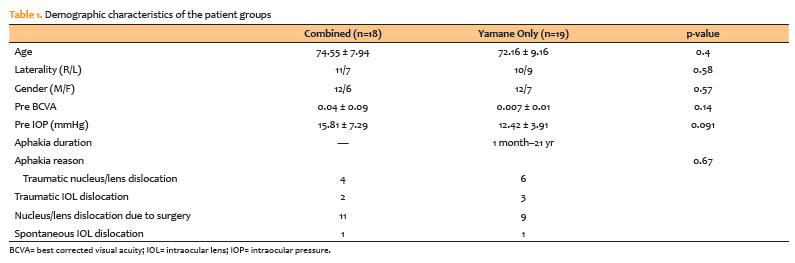
There were 18 patients in the Yamane with PPV Group and 19 in the Yamane-only Group. Age and gender distributions were not significantly different between the groups (age: with PPV: 74.55 ± 7.94, Yamane-only: 72.16 ± 9.16, p=0.4; gender [M/F]: with PPV: 12/6, Yamane-only: 12/7, p=0.57). Preoperative BCVA and IOP were also not significantly different (BCVA: with PPV: 0.04 ± 0.09, Yamane-only: 0.07 ± 0.01, p=0.14; IOP: with PPV: 15.82 ± 7.29, Yamane-only: 12.42 ± 3.91, p=0.091). The causes of aphakia were similar between the groups. The duration of aphakia ranged from 1 month to 21 yr in the Yamane-only group (Table 1).
Postoperatively, BCVA, IOP, and spherical equivalent were not significantly different between the groups (Table 2). There was no difference between the groups in terms of final IOL position (p=0.73). The mean follow-up time was 9.94 ± 2.56 months in the PPV group and 10.68 ± 3.63 months in the Yamane-only group (p=0.78).
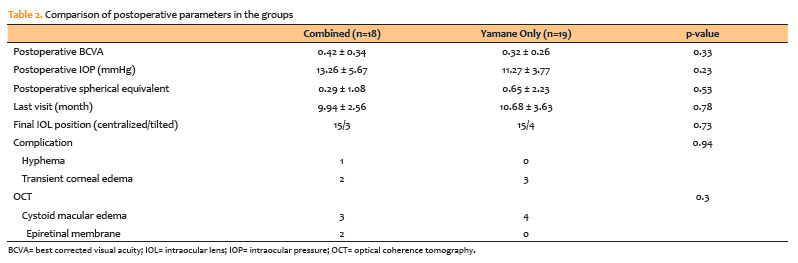
Hyphema was observed in one patient, and transient corneal edema in two patients in the PPV group. In the Yamane-only group, corneal edema was observed in three patients (p=0.94). Based on OCT findings, cystoid macular edema was detected in three patients in the PPV group and four patients in the Yamane-only group, while epiretinal membrane was observed only in two patients in the PPV group (p=0.3).
DISCUSSION
In this study, we did not find any significant differences between patients who underwent the Yamane procedure simultaneously with PPV and those who underwent the Yamane procedure alone after previous PPV in terms of postoperative BCVA, IOP, spherical equivalent, final IOL position, complications, and OCT findings.
The Yamane scleral fixation technique was first described as a combined procedure with PPV by Shin Yamane(2). The author suggested that the procedure can also be performed with anterior vitrectomy; however, surgeons should avoid retinal tears caused by vitreous traction and be cautious of possible hypotony. According to another study, the main advantage of the combined procedure is the ability to manage concomitant posterior segment conditions(7). In a study comparing PPV and anterior vitrectomy for vitreous management, no significant differences in postoperative outcomes were found between the two techniques. However, in the PPV group, one macular hole and one intraoperative retinal detachment were treated, whereas postoperative retinal detachment occurred in the anterior vitrectomy group due to an undetected retinal tear(6).
One advantage of combining the procedure with PPV is stabilization of intraocular pressure during surgery, particularly during sclerotomy and needle manipulation. Without infusion, the need for viscoelastic material may increase unless an anterior chamber maintainer is used.
Postoperative refractive status is another important consideration. The causes of aphakia are diverse and include complications during cataract surgery, spontaneous or traumatic IOL or lens dislocation, and other traumatic events. Ocular conditions and associated complications, such as vitreous hemorrhage or retinal detachment, may make accurate IOL power calculation difficult. Mutoh et al.(8) reported acceptable postoperative refractive outcomes in postvitrectomy eyes undergoing scleral fixation of IOL. Although no previous study has specifically evaluated the Yamane technique in postvitrectomy eyes for direct comparison with our study, our refractive results may support the reliability of IOL power calculation in such cases.
Good visual outcomes and refractive status are generally associated with well-centered IOLs. IOL tilt is more commonly observed in scleral-sutured fixation compared with in-the-bag implantation(9). However, no association has been found between IOL tilt and postoperative astigmatism or visual outcomes(10). In our study, slit-lamp biomicroscopy revealed tilted IOLs in 16.66%–21.05% of cases, with no significant difference between the groups. We did not compare visual outcomes or spherical equivalents between tilted and non-tilted IOLs due to the small sample size.
Completing all procedures in a single step is desirable; however, combined approaches may prolong surgical time and increase the risk of complications. These combined procedures are often required in traumatic cases. Even with in-the-bag IOL implantation, complications such as fibrinous uveitis, synechiae, pupillary capture, retinal detachment, and other posterior segment issues may occur(11). Therefore, surgeons may prefer secondary IOL implantation procedures. However, there is no clear consensus regarding the optimal timing of secondary surgery(12).
The main limitations of this study are its retrospective design and small sample size.
In conclusion, this study compared two approaches to the Yamane technique to evaluate their relative advantages and disadvantages. As no significant differences in safety or efficacy were observed between the groups, the choice of surgical approach should be guided by the surgeon’s experience and the patient’s ocular and systemic condition.
AUTHOR CONTRIBUTIONS:
Significant contribution to conception and design: Mahmut Oğuz Ulusoy, Ayna Sarıyeva-İsmayilov. Data Acquisition: Mahmut Oğuz Ulusoy, Ayna Sarıyeva-İsmayilov, Muhammed Yelkovan, Cansu Erseven. Data Analysis and Interpretation: Mahmut Oğuz Ulusoy, Ayna Sarıyeva-İsmayilov, Muhammed Yelkovan. Manuscript Drafting: Mahmut Oğuz Ulusoy. Significant intellectual content revision of the manuscript: Mahmut Oğuz Ulusoy. Final approval of the submitted manuscript: Mahmut Oğuz Ulusoy, Ayna Sarıyeva-İsmayilov, Muhammed Yelkovan, Cansu Erseven. Statistical analysis: Mahmut Oğuz Ulusoy. Obtaining funding: not applicable. Supervision of administrative, technical, or material support: Mahmut Oğuz Ulusoy. Research group leadership: Mahmut Oğuz Ulusoy.
REFERENCES
1. Bastawrous A, Parkes C, Prasad S. Choices in correction of aphakia during vitrectomy. Ophthalmologica. 2011;226(Suppl 1):46-52.
2. Yamane S, Sato S, Maruyama-Inoue M, Kadonosono K. Flanged intrascleral intraocular lens fixation with double-needle technique. Ophthalmology. 2017;124(8):1136-42.
3. Sternfeld A, Taranum Basith SS, Kurup SP, Basti S. Secondary intraocular lens implantation using the flanged intrascleral fixation technique in pediatric aphakia: case series and review of literature. J AAPOS. 2020;24(5):286.e1-286.e6.
4. Nowomiejska K, Haszcz D, Onyszkiewicz M, Choragiewicz T, Czarnek-Chudzik A, Szpringer-Wabicz A, et al. Double-needle Yamane technique using flanged haptics in ocular trauma-a retrospective survey of visual outcomes and safety. J Clin Med. 2021;10(12):2562.
5. Cho BJ, Yu HG. Surgical outcomes according to vitreous management after scleral fixation of posterior chamber intraocular lenses. Retina. 2014;34(10):1977-84.
6. Tang Y, Yao S, Chu Y, Han Q. Vitreous management in Yamane’s technique for crystalline lens dislocation: anterior vitrectomy or PPV? BMC Ophthalmol. 2023;23(1):466.
7. Shelke K, Rishi E, Rishi P. Surgical outcomes and complications of sutureless needle-guided intrascleral intraocular lens fixation combined with vitrectomy. Indian J Ophthalmol. 2021;69(9):2317-20.
8. Mutoh T, Matsumoto Y, Chikuda M. Scleral fixation of foldable acrylic intraocular lenses in aphakic post-vitrectomy eyes. Clin Ophthalmol. 2010;5:17-21.
9. Hayashi K, Hayashi H, Nakao F, Hayashi F. Intraocular lens tilt and decentration, anterior chamber depth, and refractive error after trans-scleral suture fixation surgery. Ophthalmology. 1999;106(5):878-82.
10. Kemer Atik B, Altan C, Agca A, Kirmaci A, Yildirim Y, Genc S, et al. The effect of intraocular lens tilt on visual outcomes in scleral-fixated intraocular lens implantation. Int Ophthalmol. 2020;40(3):717-24.
11. He T, You C, Chen S, Meng X, Liu Y, Yan H. Secondary sulcus-fixed foldable IOL implantation with 25-g infusion in patients with previous PPV after open-globe injury. Eur J Ophthalmol. 2017;27(6):786-90.
12. Riazi M, Moghimi S, Najmi Z, Ghaffari R. Secondary Artisan-Verysise intraocular lens implantation for aphakic correction in post-traumatic vitrectomized eye. Eye (Lond). 2008;22(11):1419-24.
Data Availability Statement: The datasets produced and/or analyzed in this study can be provided to referees upon request.
Edited by
Editor-in-Chief: Newton Kara-Júnior
Associate Editor: Richard Y. Hida
Submitted for publication:
September 9, 2025.
Accepted for publication:
March 26, 2026.
Approved by the following research ethics committee: Bursa Yüksek İhtisas Research and Training Hospital (2011-KAEK-25-2023/12-07)
Funding: This study received no specific financial support.
Disclosure of potential conflicts of interest: The authors declare no potential conflicts of interest.

How to cite this article:
 ABO is licensed under a Creative Commons Attribution-NonComercial 4.0 Internacional.
ABO is licensed under a Creative Commons Attribution-NonComercial 4.0 Internacional.