Arq. Bras. Oftalmol. 2026; 89 (4): 10.5935/0004-2749.2024-0409
Total: 16
Correlation between tear crystallization and corneal esthesiometry in patients with Sjögren's syndrome
Karolyna Andrade de Carvalho1; Lucas Paolera1; Bernardo Kaplan Moscovici2,3; Luiz Antônio Brito1; Luiz Felipe Ramos Bueno1; Sergio Felberg1
DOI: 10.5935/0004-2749.2024-0409
ABSTRACT
PURPOSE: The purpose of this study is to look into the relationship between tear film osmolarity, tear crystallization, and corneal esthesiometry findings in Sjögren's syndrome patients.
METHODS: This cross-sectional observational study included 43 eyes from patients with a confirmed diagnosis of Sjögren's syndrome. Tear osmolarity was measured with an iPen osmometer, tear crystallization was graded using Roland's classification, and corneal sensitivity was evaluated with a Cochet–Bonnet aesthesiometer. Ocular symptoms were assessed using the Ocular Surface Disease Index questionnaire. Patients who had undergone keratoplasty or worn contact lenses within 4 hours of testing were excluded.
RESULTS: The cohort's mean tear osmolarity was 292.5±15.0 mOsm/L (median: 293 mOsm/L, IQR: 17.5). There was no significant difference between patients with primary Sjögren's syndrome (mean: 289.4 mOsm/L) and those with secondary Sjögren's syndrome (mean: 294.5 mOsm/L; p=0.413). Tear crystallization patterns were more severe in patients with primary Sjögren's syndrome (mean: 3.25, median: 3.5, IQR: 1.25) than in those with secondary Sjögren's syndrome (mean: 3.19, median: 3.0, IQR: 1.0), though the difference was not statistically significant (p=0.87). Corneal sensitivity was reduced by 3.5±1.7 mm (median: 4.0 mm, IQR: 2.13). Tear crystallization has a significant negative correlation with corneal sensitivity (r=−0.313, p=0.041), suggesting that poorer tear quality leads to decreased corneal sensitivity.
CONCLUSION: Tear crystallization patterns and corneal sensitivity were found to be significantly correlated in Sjögren's syndrome patients. The findings also indicate that systemic medication use may affect tear film quality.
Keywords: Sjogren's syndrome, Tear crystallization, Dry eye disease, Cornea, Tears, Osmolarity
INTRODUCTION
Sjögren's syndrome (SS) is a chronic autoimmune disorder that primarily affects the exocrine glands, specifically the lacrimal and salivary glands(1), causing the classic symptoms of dry eye disease (DED) and xerostomia. Several questionnaires and diagnostic tests have been developed to aid in the evaluation of DED; however, no single test has been widely accepted as the gold standard for diagnosis(1-19).
The American College of Rheumatology and the European League Against Rheumatism developed diagnostic criteria for dry eye that include Schirmer's test (<5 mm in 5 min) and/or fluorescein staining (van Bijsterveld score >4)(1).
In 2017, the Tear Film and Ocular Surface Society Dry Eye Workshop II (TFOS DEWS II) defined dry eye as a multifactorial disease of the ocular surface characterized by loss of tear-film homeostasis and accompanied by ocular symptoms. It is associated with tear film instability, hyperosmolarity, ocular surface inflammation and damage, and neurosensory abnormalities(11-17).
To diagnose DED, the most commonly used tests are tear film break-up time, corneal staining with fluorescein dye, conjunctival staining with lissamine green or rose bengal dyes, and the Schirmer test. Other tests, such as evaluation of tear osmolarity (TO), tear crystallization (TC), and corneal aesthesiometry (CAE), are also used. However, there is still no consensus on which ones should be used. Furthermore, some tests, such as staining scores, can affect classification due to observer bias and variability when performed by different examiners (1-17).
The primary cause of dry eye has been identified as tear film hyperosmolarity, which can cause inflammation and ocular surface damage. The FDA has approved new portable devices that are innocuous and pose no risk to patients. These devices allow measurement of tear TO in very small volumes and can be performed during a routine appointment. Several studies have found that increased tear osmolarity and/or measurement variability indicate dry eye due to tear film instability. According to some studies, this measurement has high sensitivity and specificity, making it useful for diagnosing and monitoring patients with DED(1-17).
The ferning test, also called the TC test, assesses the quality of the tear film. It entails observing the TC patterns that appear when a small sample of the film is removed from the bottom of the patient's eye bag(4).
A Cochet-Bonnet aesthesiometer was used for the CAE test. In this test, a thin nylon filament of varying lengths is placed on the center of the cornea, and the patient is asked to indicate whether they feel a sensation of touch as the filament is shortened. It is a quick test used to assess corneal tactile sensitivity when there is a possibility of decreased sensitivity. Values <6 indicate that the test is below normal(20,21).
The Ocular Surface Disease Index is a reliable and validated questionnaire that is widely used in clinical and research settings. It is part of the TFOS DEWS diagnostic guidelines for DED. The OSDI assesses DED severity by measuring the frequency and severity of symptoms, as well as their impact on daily activities. It effectively complements clinical assessments by assisting in correlating subjective symptoms with objective findings(14).
This study investigated the relationships among TO, TC, and CAE in SS patients. It also aimed to link systemic medication and the OSDI questionnaire to the previously mentioned tests.
METHODS
Study design
The Research Ethics Committee of Santa Casa de Misericórdia de São Paulo (42220820.0.0000.5479) approved this cross-sectional, observational, and descriptive case series study in accordance with the principles of the Declaration of Helsinki. All participants provided informed consent before being included in the study.
The study included patients aged 18 and older who had been diagnosed with SS using the American College of Rheumatology criteria. As an observational case series, the study only included patients with a confirmed diagnosis of SS to assess correlations within this population rather than comparing them to a healthy control group.
Inclusion and exclusion criteria
Patients were eligible if they met the diagnostic criteria for SS and were at least 18 yr old. Exclusion criteria included DED caused by other factors, contact lenses, glaucoma, or the inability to provide consent.
Following the evaluation, we excluded the only male patient to avoid the effect of gender on osmolarity and crystallization.
Randomization
Because of the study's case series design, no randomization was used to select patients. To capture the clinical spectrum of the disease, all patients with a confirmed diagnosis of SS who met the inclusion criteria during the study period were included in the analysis.
Data collection and ophthalmic examinations
The information gathered included age, gender, medical history, clinical diagnosis, and duration of SS. The hormonal status of female participants was not specifically recorded, and the duration of SS was determined retrospectively from medical records. To avoid influencing the results, patients should not use eye drops for at least 4 h before the test.
All patients underwent a thorough ophthalmological examination, which included assessments of the tear film and corneal sensitivity, as well as a subjective evaluation of ocular surface symptoms using the OSDI.
The physicians who evaluated the dry eye tests were not aware of the ophthalmic examination or the patient's diagnosis.
Exam description
TO: was measured with the iPen osmometer. A 50-nL tear sample was collected from both eyes' conjunctival fornices, and the device measured its electrical impedance. Results >300 mOsm/L indicated hyperosmolarity.
TC: The tear film's quality was evaluated using the ferning test. Tear samples were collected from the conjunctival fornix using a capillary glass tube, transferred to a glass slide, dried at room temperature for 10 min, and examined under a polarized light microscope. Roland's model was used to classify crystallization patterns into four stages. Stage I consists of multi-branched crystals with no gaps between branches, indicating optimal tear quality; Stage II has shorter branches with moderate gaps, indicating mild tear film impairment; Stage III has sparse branching with large gaps, indicating significant tear instability; and Stage IV has lumped crystals with minimal branching, indicating severe tear dysfunction. In this study, patterns corresponding to Stages III and IV indicated impaired tear film quality, which is consistent with the tear instability seen in advanced Sjögren's syndrome.
Corneal sensitivity was assessed using the Cochet-Bonnet aesthesiometer. The nylon filament was applied to the central cornea, and the length was reduced in 0.5-mm increments until the patient felt a tactile sensation. Values <6.0 mm were considered abnormal, indicating reduced corneal sensitivity, a common finding in SS patients.
A trained examiner administered the OSDI questionnaire to assess the severity of dry eye symptoms and correlate subjective responses with objective findings such as TO and corneal sensitivity. The test is a 12-item tool that has been validated and is widely used in clinical and research settings. It has a score range of 0 to 100. All examinations were performed in the morning, and patients were told not to use eye drops on the day of the test to avoid interfering with the results.
Statistical analysis
Statistical analyses were carried out using SPSS V26, Minitab 21.2, and Microsoft Excel 2010. P-values <0.05 were considered significant. The Kolmogorov-Smirnov test revealed that the data were not normally distributed, necessitating the use of non-parametric tests for reliable analysis.
The Mann-Whitney U test was used to compare patients with primary and secondary Sjögren's syndrome, as well as those who used and did not use systemic medications. The relationships between TO, TC, corneal sensitivity, and OSDI scores were examined using Spearman's rank correlation coefficient, with negative coefficients indicating that worse crystallization was associated with decreased sensitivity.
RESULTS
Sample distribution
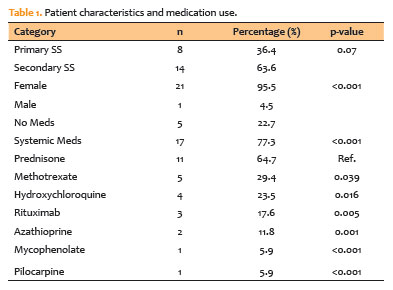
The study involved 22 patients (43 eyes) diagnosed with SS, with a mean age of 55.8 ± 5.0 yr (range: 48-63). The majority of participants were female (95.5%, n=21); the single male patient was excluded to avoid potential gender bias in osmolarity and crystallization. This female predominance is consistent with the established epidemiology of SS, which affects women in more than 90% of cases.
The cohort comprised 61.9% (n=13) with secondary SS and 38.1% (n=8) with primary SS. There was no statistically significant difference in the distribution of primary and secondary SS (p=0.070). The average disease duration was not recorded, which limits the interpretation of the results (Table 1).
Ophthalmological examination
All patients underwent a thorough ophthalmological examination, which included slit-lamp biomicroscopy, tear film evaluation, and corneal sensitivity testing with a Cochet-Bonnet esthesiometer. The OSDI was used to determine the severity of dry eye symptoms, with scores divided into four categories: normal, mild, moderate, and severe. In this study, 27.28% of the patients had normal OSDI scores, 22.72% had mild impairment, 45.45% had moderate impairment, and 4.55% had significant impairment.
Tear osmolarity
TO was measured with an iPen osmometer, yielding values of 280 and 320 mOsm/L. Interestingly, osmolarity levels remained within the normal range (mean: 292.5 ± 15.0 mOsm/L), despite expectations for DED associated with SS. Tables 2 and 3 show that there was no significant correlation between tear osmolarity and TC (r=−0.130, p=0.408) or corneal sensitivity (r=−0.228, p=0.142).


Tear crystallization
TC was evaluated using the Roland classification system, which identifies four crystallization patterns. Most patients showed signs of poor tear film quality (Stages III and IV). A statistically significant negative correlation was found between TC and corneal sensitivity (r=−0.313, p=0.041), indicating that as tear crystallization progressed, corneal sensitivity decreased (Table 2).
Corneal sensitivity
Corneal sensitivity was measured using a Cochet-Bonnet esthesiometer, and values <6.0 mm indicated reduced sensitivity. The average corneal sensitivity in this cohort was 3.5 ± 1.7 mm, with significant differences between patients with primary and secondary SS. However, no statistically significant differences were found between primary and secondary SS in terms of sensitivity (p=0.156) or crystallization (p=0.787; Table 2).
Systemic medication use
Patients frequently used systemic medications, with 72.72% (n=16) using at least one topical ocular medication to manage their dry eyes. All patients used preservative-free artificial tears made of sodium hyaluronate or sodium carmellose five to eight times daily, and 18.75% (n=3) were taking topical immunomodulators like cyclosporine. Prednisone was the most commonly used systemic medication among the 17 patients (64.7%, n=11), followed by methotrexate (29.4%, n=5). There was a significant difference in TC between patients who took systemic medications and those who did not. Table 1 shows that those taking systemic medications had worse tear crystallization patterns (mean=3.41) than those not on systemic treatment (mean=2.44; p=0.002). However, these two groups showed no significant difference in osmolarity or corneal sensitivity.
TC had a significant negative correlation with corneal sensitivity (r=−0.313, p=0.041), while tear osmolarity levels were normal (mean: 292.5 ± 15.0 mOsm/L). There was no significant correlation between osmolarity and other parameters. Patients with more severe TC patterns had reduced corneal sensitivity.
DISCUSSION
DED is frequently diagnosed based on ocular symptoms and clinical signs observed during ophthalmic examinations, which can serve as an early indicator of SS. Although DED is typically symptomatic, studies have shown that more than 40% of people with objective evidence of the disease are asymptomatic, highlighting DED diagnostic complexities(1,11,17). OSDI tools are critical for bridging this gap because they capture subjective symptom variability and complement objective clinical assessments. Our study investigated the relationships among TO, TC, CAE, and systemic medication use in SS patients to understand ocular surface dysfunction in this population better.
Our cohort's TO levels were within the normal range (mean: 292.5 ± 15.0 mOsm/L), unlike previous studies that linked elevated TO to DED in SS. For example, Tomlinson et al. and Na et al. found significantly higher TO in patients with SS, frequently exceeding 316 mOsm/L, which is associated with severe tear film instability. This disparity could be explained by our participants' frequent use of systemic immunosuppressive medications, which could stabilize tear film homeostasis and reduce hyperosmolarity, as previously suggested by Moscovici et al. Furthermore, differences in methodologies, particularly the use of the iPen osmometer in our study, may contribute to variability, as its sensitivity for detecting subtle changes in osmolarity differs from that of other validated devices. Furthermore, methodological differences may contribute to variability, particularly the use of the iPen osmometer, which, despite being FDA-approved, portable, and requiring minimal tear volume, has lower sensitivity than other validated devices. This limitation may explain some of the normal osmolarity values observed in our cohort, but its practicality makes it appropriate for routine clinical use(5,20-22).
While TO showed no significant correlation with other parameters in our study, TC emerged as a reliable indicator of tear film instability, with advanced TC stages negatively correlated with CAE (r=-0.313, p=0.041). This finding reinforces the importance of TC detecting ocular surface dysfunction in SS patients. Felberg et al. previously validated the reproducibility of TC classification in SS patients, demonstrating that higher TC stages are significantly associated with ocular surface inflammation and poor tear quality. These observations align with our results and further underscore the utility of TC as a diagnostic tool for DED in SS(4,23-25).
The relationship between TC and CAE observed in our study supports the hypothesis that chronic inflammation in SS causes corneal nerve desensitization, reducing nociceptive signaling and resulting in fewer symptoms despite severe ocular surface damage. This finding is consistent with those of Tuominen et al.(24), who used confocal microscopy to show altered corneal nerve morphology and reduced subbasal plexus density in SS patients. Similarly, Luzu et al. found neuromas and inflammatory infiltrates in the corneal nerves of SS patients, which likely contribute to reduced corneal sensitivity and complicate the disease phenotype. These structural changes explain the significant negative correlation between TC and CAE observed in our cohort(23-25).
Although the differences between primary and secondary SS were not statistically significant, our results suggested a trend toward more advanced tear crystallization and lower corneal sensitivity in primary SS (mean CAE, 3.2±1.5 mm; 71.4% of patients in TC stages III-IV) compared with secondary SS (63.2% in TC stages III-IV). Given the small sample size, these findings should be interpreted with caution. Cardigos et al. reported similar findings, observing increased nerve damage and inflammatory markers in primary SS. The increased use of systemic immunosuppressive therapy in patients with secondary SS may help explain this trend, as such treatments can reduce inflammatory damage and preserve corneal sensitivity(5,20-27).
Kim et al. found that SS patients had more pronounced ocular surface signs but fewer symptoms than non-SS DED patients. Their findings revealed that CAE values were comparable between the SS and non-SS groups, implying that corneal sensitivity is affected differently in severe DED cases. While our findings showed a significant correlation between TC and CAE, this disparity could be due to differences in patient populations, disease severity, or methodologies used. Furthermore, our observation of reduced corneal sensitivity in patients with advanced TC stages supports the hypothesis that chronic, prolonged inflammatory stimulation may desensitize polymodal nociceptors, resulting in fewer symptoms despite severe tear film abnormalities (23-25).
TO, while widely recognized as a defining feature of DED, did not fully capture the complexities of ocular surface dysfunction in our cohort. However, combining TO with other diagnostic tools, such as TC and CAE, improves diagnostic accuracy and provides a more comprehensive assessment of SS-associated DED. For example, Alves et al. demonstrated that integrating TO with TBUT and Schirmer's test improved sensitivity and specificity, highlighting the value of multimodal approaches in diagnosing DED. Fenga et al. also found that TO had greater discriminative capacity than the OSDI among video display terminal workers, supporting the use of complementary diagnostic methods to address the multifaceted nature of DED (5,22-30).
Clinically, our findings highlight the importance of combining objective and subjective assessments when diagnosing DED. The significant correlation between TC and CAE highlights TC's usefulness as a reliable indicator of tear film quality and neurosensory dysfunction in SS patients. The effect of systemic medications on TC emphasizes the need for a multidisciplinary approach to managing SS-associated DED that includes both systemic and ocular treatments.
This study has limitations that should be addressed. The small, single-center sample size limits the statistical power of subgroup analyses and their generalizability. The absence of standardized data on disease duration and hormonal status could have also influenced tear film parameters and neurosensory function. Furthermore, the lack of a control group and the use of the iPen osmometer, which has lower sensitivity than other devices, could have influenced the findings. These factors should be considered in future multicenter studies.
In conclusion, this study found significant correlations between TC and corneal sensitivity, as well as an effect of systemic medication use on tear film quality in patients with SS. While TO showed no significant associations, crystallization and esthesiometry emerged as the most reliable indicators of ocular surface dysfunction in this cohort. These findings emphasize the importance of combining multiple diagnostic tools when assessing SS-associated dry eye, as well as the need for additional research to confirm these results and refine diagnostic strategies.
AUTHORS' CONTRIBUTION:
Substantial Contribution to Conception and Design: Karolyna Andrade de Carvalho, Luiz Antônio Brito, Luiz Felipe Ramos Bueno, Sergio Felberg.
Acquisition of Data: Karolyna Andrade de Carvalho, Lucas Paolera.
Analysis and Interpretation of Data: Karolyna Andrade de Carvalho, Bernardo Kaplan Moscovici.
Drafting of the Manuscript: Karolyna Andrade de Carvalho, Lucas Paolera, Bernardo Kaplan Moscovici.
Critical Revision of the Manuscript for Important Intellectual Content: Luiz Antônio Brito, Luiz Felipe Ramos Bueno,Sergio Felberg.
Final Approval of the Submitted Manuscript: Karolyna Andrade de Carvalho, Lucas Paolera, Bernardo Kaplan Moscovici, Luiz Antônio Brito, Luiz Felipe Ramos Bueno, Sergio Felberg.
Statistical Analysis: Bernardo Kaplan Moscovici.
Obtaining funding: not applicable.
Administrative, Technical, or Material Support Supervision: Karolyna Andrade de Carvalho, Lucas Paolera, Bernardo Kaplan Moscovici.
Research Group Leadership: Luiz Antônio Brito, Luiz Felipe Ramos Bueno, Sergio Felberg.
REFERENCES
1. Kuklinski E, Asbell PA. Sjogren's syndrome from the perspective of ophthalmology. Clin Immunol. 2017;182:55-61.
2. Felberg S, Dantas PE. [Sjögren's syndrome: diagnosis and treatment]. Arq Bras Oftalmol. 2006;69(6):959-63. Portuguese;
3. Barboza MN, Barboza GN, de Melo GM, Sato E, Dantas MC, Dantas PE, et al. [Correlation between signals and symptoms of dry eye in Sjögren's syndrome patients]. Arq Bras Oftalmol. 2008;71(4):547-52. Portuguese.
4. Felberg S, Cordeiro H, Sato EH, Martini Filho D, Nishiwaki-Dantas MC, Endo RM, et al. [Reproducibility of the classification of ocular ferning patterns in Sjogren's syndrome patients]. Arq Bras Oftalmol. 2008;71(2):228-33. Portuguese.
5. Willcox MD, Argüeso P, Georgiev GA, Holopainen JM, Laurie GW, Millar TJ, et al. TFOS DEWS II Tear Film Report. Ocul Surf. 2017;15(3):366-403.
6. Ibrahim OM, Dogru M, Takano Y, Satake Y, Wakamatsu TH, Fukagawa K, et al. Application of visante optical coherence tomography tear meniscus height measurement in the diagnosis of dry eye disease. Ophthalmology. 2010; 117(10):1923-9.
7. Epstein SP, Gadaria-Rathod N, Wei Y, Maguire MG, Asbell PA. HLA-DR expression as a biomarker of inflammation for multicenter clinical trials of ocular surface disease. Exp Eye Res. 2013;111:95-104.
8. Barabino S, Montaldo E, Solignani F, Valente C, Mingari MC, Rolando M. Immune response in the conjunctival epithelium of patients with dry eye. Exp Eye Res. 2010;91(4):524-9.
9. Adatia FA, Michaeli-Cohen A, Naor J, Caffery B, Bookman A, Slomovic A. Correlation between corneal sensitivity, subjective dry eye symptoms, and corneal staining in Sjögren's syndrome. Can J Ophthalmol. 2004;39(7):767-71.
10. Tuominen IS, Konttinen YT, Vesaluoma MH, Moilanen JA, Helintö M, Tervo TM. Corneal innervation and morphology in primary Sjögren's syndrome. Invest Ophthalmol Vis Sci. 2003;44(6):2545-9.
11. Craig JP, Nichols KK, Akpek EK, Caffery B, Dua HS, Joo CK, et al. TFOS DEWS II Definition and Classification Report. Ocul Surf. 2017;15(3):276-83.
12. Craig JP, Nelson JD, Azar DT, Belmonte C, Bron AJ, Chauhan SK, et al. TFOS DEWS II Report Executive Summary. Ocul Surf. 2017;15(4):802-12.
13. Jones L, Downie LE, Korb D, Benitez-Del-Castillo JM, Dana R, Deng SX, et al. TFOS DEWS II Management and Therapy Report. Ocul Surf. 2017;15(3):575-628.
14. Wolffsohn JS, Arita R, Chalmers R, Djalilian A, Dogru M, Dumbleton K et al. TFOS DEWS II Diagnostic Methodology report. Ocul Surf. 2017;15(3):539-74.
15. Bron AJ, de Paiva CS, Chauhan SK, Bonini S, Gabison EE, Jain S et al. TFOS DEWS II pathophysiology report. Ocul Surf. 2017;15(3):438-510.
16. Stapleton F, Alves M, Bunya VY, Jalbert I, Lekhanont K, Malet F et al. TFOS DEWS II Epidemiology Report. Ocul Surf. 2017;15(3):334-65.
17. Moscovici BK, Holzchuh R, Sakassegawa-Naves FE, Hoshino-Ruiz DR, Albers MB, Santo RM, et al. Treatment of Sjögren's syndrome dry eye using 0.03% tacrolimus eye drop: prospective double-blind randomized study. Cont Lens Anterior Eye. 2015;38(5):373-8.
18. Moscovici BK, Holzchuh R, Chiacchio BB, Santo RM, Shimazaki J, Hida RY. Clinical treatment of dry eye using 0.03% tacrolimus eye drops. Cornea. 2012;31(8):945-9.
19. Sanchez V, Dobzinski N, Fox R, Galor A. Rethinking Sjögren Beyond Inflammation: Considering the Role of Nerves in Driving Disease Manifestations. Eye Contact Lens. 2024;50(5):200-7.
20. Kim M, Chun YS, Kim KW. Different perception of dry eye symptoms between patients with and without primary Sjogren's syndrome. Sci Rep. 2022;12(1):2172.
21. Crabtree JR, Tannir S, Tran K, Boente CS, Ali A, Borschel GH. Corneal nerve assessment by aesthesiometry: history, advancements, and future directions. Vision (Basel). 2024;8(2):34.
22. Luzu J, Labbé A, Réaux-Le Goazigo A, Rabut G, Liang H, Dupas B et al. In vivo confocal microscopic study of corneal innervation in Sjögren's Syndrome with or without small fiber neuropathy. Ocul Surf. 2022;25:155-62.
23. Cardigos J, Barcelos F, Carvalho H, Hipólito D, Crisóstomo S, Vaz-Patto J, et al. Tear meniscus and corneal sub-basal nerve plexus assessment in primary Sjögren syndrome and sicca syndrome patients. Cornea. 2019;38(2):221-8.
24. Fenga C, Aragona P, Di Nola C, Spinella R. Comparison of ocular surface disease index and tear osmolarity as markers of ocular surface dysfunction in video terminal display workers. Am J Ophthalmol. 2014;158(1):41-48.e2.
25. Khanal S, Tomlinson A, McFadyen A, Diaper C, Ramaesh K. Dry eye diagnosis. Invest Ophthalmol Vis Sci. 2008;49(4):1407-14.
26. Tomlinson A, McCann LC, Pearce EI. Comparison of human tear film osmolarity measured by electrical impedance and freezing point depression techniques. Cornea. 2010;29(9):1036-41.
27. Tomlinson A, Khanal S, Ramaesh K, Diaper C, McFadyen A. Tear film osmolarity: determination of a referent for dry eye diagnosis. Invest Ophthalmol Vis Sci. 2006;47(10):4309-15.
28. Alves M, Reinach PS, Paula JS, Vellasco e Cruz AA, Bachette L, Faustino J et al. Comparison of diagnostic tests in distinct well-defined conditions related to dry eye disease. PLoS One. 2014;9(5):e97921.
29. Moscovici BK, Cesar AS, Nishiwaki-Dantas MC, Mayor SA, Marta AC, Marques JC. Dermatoceratoconjuntivite atópica em pacientes do Ambulatório de Dermatologia Infanto-Juvenil em centro de referência. Dermatoceratoconjunctivitis in patients of the pediatric dermatology ambulatory in a reference center. Arq Bras Oftalmol. 2009;72(6):805-10. Portuguese.
30. Vedovato MA, Do Carmo TQM, Rios LC, Corrêa VC, Oliveira FR, Capelanes NC, et al. Use of topical tacrolimus in ophthalmology: nonsystematic review. Pan Am J Ophthalmol. 2020;2(1):36.
Submitted for publication:
December 20, 2024.
Accepted for publication:
April 11, 2026.
Approved by the following research ethics committee: Santa Casa de Misericórdia de São Paulo (CAAE: 42220820.0.0000.5479).
Data Availability Statement: The datasets generated and/or analyzed during the current study are available from the corresponding author upon reasonable request and subject to appropriate justifications.
Edited by
Editor-in-Chief: Newton Kara-Júnior
Associate Editor: José Álvaro Pereira Gomes
Funding: This study received no specific financial support.
Disclosure of potential conflicts of interest: The authors declare no potential conflicts of interest.

How to cite this article:
 ABO is licensed under a Creative Commons Attribution-NonComercial 4.0 Internacional.
ABO is licensed under a Creative Commons Attribution-NonComercial 4.0 Internacional.