Arq. Bras. Oftalmol. 2023;86 (5 )
:1-6
| DOI: 10.5935/0004-2749.20230070
Abstract
Objetivo: A refração pós-operatória na cirurgia moderna de catarata por microincisão ganha ainda mais importância em pacientes com cirurgia prévia de ceratomileuse in situ assistida por laser (LASIK). As alterações astigmáticas induzidas cirurgicamente nesses olhos podem diferir não apenas em magnitude, mas também em direção em comparação com córneas virgens. O objetivo deste estudo foi comparar as alterações astigmáticas induzidas cirurgicamente após cirurgia de catarata por microincisão entre córneas pós-LASIK e olhos virgens.
Métodos: Foi revisada uma série de casos de cirurgia de catarata por microincisão em olhos com e sem cirurgia LASIK anterior. Os dados demográficos, o comprimento axial no momento da cirurgia de catarata, a espessura central da córnea, os valores esféricos e cilíndricos, as leituras da ceratometria e o astigmatismo corneano posterior pós-operatório foram avaliados retrospectivamente. O método Alpins modificado foi usado para análise vetorial astigmática e foram avaliados o astigmatismo basal, o astigmatismo induzido cirurgicamente, o vetor de diferença, o efeito de achatamento e o torque.
Resultados: Ao todo, 42 olhos de 24 indivíduos foram avaliados. O Grupo I consistiu em 14 olhos com LASIK prévio; o Grupo II incluiu 28 olhos sem qualquer cirurgia refrativa. A média da espessura corneana central pré-operatória no Grupo I foi significativamente mais fina (p=0,012). Não houve diferença significativa no astigmatismo basal entre os grupos em termos de magnitude e vetores de potência. Após a cirurgia de catarata por microincisão, não houve diferenças significativas nos valores médios esféricos, cilíndricos e leituras médias de ceratometria (todos com p>0,05). No entanto, o astigmatismo induzido cirurgicamente e o vetor de diferença foram significativamente maiores no componente do vetor J45 em olhos pós-LASIK, e o efeito de aumento da inclinação pela cirurgia de catarata por microincisão nas córneas pós-LASIK foi significativo em comparação com olhos virgens (p=0,001, p=0,002 e p=0,018, respectivamente).
Conclusões: A cirurgia de catarata aumentou a inclinação das córneas em ambos os grupos, sendo esse aumento significativamente maior nos olhos pós-LASIK. Certamente, a topografia da córnea antes da cirurgia de catarata é particularmente útil para fornecer interpretações mais precisas do astigmatismo induzido cirurgicamente.
Keywords: Cirurgia de catarata; Ceratomileuse; excimer laser in situ; Cirurgia refrativa; Astigmatismo induzido cirurgicamente; Análise vetorial.
Arq. Bras. Oftalmol. 2023;86 (3 )
:1-5
| DOI: 10.5935/0004-2749.20230031
Abstract
Objetivo: Descrever os resultados clínicos do tratamento do crescimento epitelial através da técnica de remoção manual seguido da utilização de um compressor de ar comprimido aquecido após a cirurgia de laser in situ keratomileusis (LASIK).
Métodos: Vinte olhos de 17 pacientes foram incluídos no estudo. Cada paciente havia sido submetido a cirurgia de LASIK com presença de crescimento epitelial e foi submetido a tratamento cirúrgico para sua retirada. O objetivo primário foi identificar a presença de crescimento epitelial recorrente ao final de 3 meses de seguimento. Os objetivos secundários foram as medidas de acuidade visual sem correção, acuidade visual com correção, e complicações pós-operatórias.
Resultados: Dez pacientes (58,8%) eram homens e 7 mulheres. Oito olhos de sete (41,2%) pacientes apresentavam cirurgia de LASIK primária e 12 olhos de 10 pacientes tinham cirurgia de LASIK com retratamento; dezesseis olhos (80%) utilizaram microcerátomo manual e quatro (20%) laser de femtosegundo. A média de idade no momento da cirurgia de remoção do epitélio era de 37,0 anos ± 9,3 (DP) (variando de 24 a 55 anos). Ocorreu recidiva do crescimento epithelial em dois olhos (10%) após 3 meses de seguimento. A acuidade visual sem correção antes da cirurgia era de 0,07 ± 0,09 logMAR, e após a cirurgia passou para 0,02 ± 0,04 logMAR (p=0,06). A chance (odds ration) de aparecimento do crescimento epithelial após uma reoperação de LASIK é 29,41 vezes maior do que no LASIK primário.
Conclusão: A técnica de remoção epitelial manual seguida da utilização de ar comprimido aquecido é segura e efetiva no tratamento do crescimento epitelial após LASIK. Ao final do último acompanhamento, nenhum olho apresentou perda de linhas de visão.
Keywords: Epitélio/crescimento & desenvolvimento; Endotélio corneano; Doenças da córnea; Ceratomileuse assistida por excimer laser in situ; Ceratectomia fotorrefrativa; Procedimentos cirúrgicos refrativos; Acuidade visual
Arq. Bras. Oftalmol. 2023;86 (3 )
:1-6
| DOI: 10.5935/0004-2749.20230044
Abstract
Objetivo: O setor nasal do ângulo da câmara anterior pode apresentar maior densidade de canais coletores, o que pode influenciar no resultado de cirurgias angulares. Considerando as diferenças anatômicas no ângulo da câmara anterior, comparamos os resultados das abordagens de trabeculoplastia seletiva a laser nasal e temporal de 180 graus no glaucoma de ângulo aberto.
Métodos: Revisão retrospectiva de prontuários de pacientes com glaucoma de ângulo aberto (primária, pseudoexfoliação e pigmentar), que realizaram pelo menos uma sessão de trabeculoplastia seletiva a laser de 180 graus entre dezembro/2016 e outubro/2018. O setor nasal (N1) ou temporal (T1) foi escolhido a critério do médico. Os pacientes que não apresentaram diminuição da pressão intraocular (PIO) entre 3 e 6 meses foram retratados com trabeculoplastia seletiva a laser de 180 graus no setor de ângulo oposto (T2 e N2). O principal resultado medido foi a diminuição da pressão intraocular no 6º mês de acompanhamento após a última trabeculoplastia seletiva a laser. Uma análise de regressão multivariável avaliou os fatores associados à redução da pressão intraocular após o tratamento.
Resultados: O procedimento foi realizado inicialmente em 45 olhos (N1=25, T1=20 olhos), e repetido no setor ângulo da câmara anterior oposto em 19 olhos (N2 = 11, T2 = 8 olhos). Os testes ANOVA mostraram que apenas a abordagem N1 apresentou diferença significativa na diminuição da pressão intraocular em relação a T1, N2 e T2 (p=0,0014). A pressão intraocular basal (p=0,021) e o setor ângulo da câmara anterior (N1; p=0,044) se correlacionaram com a diminuição da pressão intraocular.
Conclusão: A trabeculoplastia seletiva a laser de 180 graus realizado inicialmente no setor nasal foi associado a uma diminuição mais significativa da pressão intraocular em comparação com a abordagem temporal. Considerando as diferenças setoriais no ângulo da câmara anterior, mais estudos prospectivos são necessários para confirmar nossos achados e fornecer protocolos para trabeculoplastia seletiva a laser mais eficientes.
Keywords: Glaucoma de ângulo aberto; Terapia a laser/métodos; Pressão intraocular; Trabeculoplastia/métodos.
Arq. Bras. Oftalmol. 2025;88 (1 )
:1-8
| DOI: 10.5935/0004-2749.2023-0103
Abstract
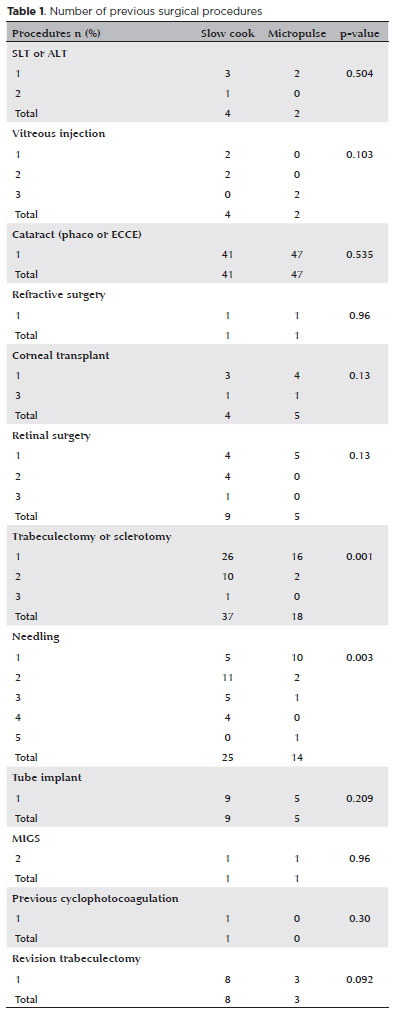
PURPOSE: This study aimed to compare the safety and effectiveness of intraocular pressure reduction between micropulse transscleral cyclophotocoagulation and “slow cook” transscleral cyclophotocoagulation in patients with refractory primary open-angle glaucoma.
METHODS: We included patients with primary open angle glaucoma with at least 12 months of follow-up. We collected and analyzed data on the preoperative characteristics and postoperative outcomes. The primary outcomes were a reduction of ≥20% of the baseline value (criterion A) and/or intraocular pressure between 6 and 21 mmHg (criterion B).
RESULTS: We included 128 eyes with primary open-angle glaucoma. The preoperative mean intraocular pressure was 25.53 ± 6.40 and 35.02 ± 12.57 mmHg in the micropulse- and “slow cook” transscleral cyclophotocoagulation groups, respectively (p<0.001). The mean intraocular pressure was reduced significantly to 14.33 ± 3.40 and 15.37 ± 5.85 mmHg in the micropulse- and “slow cook” transscleral cyclophotocoagulation groups at the last follow-up, respectively (p=0.110). The mean intraocular pressure reduction at 12 months was 11.20 ± 11.46 and 19.65 ± 13.22 mmHg in the micropulse- and “slow cook” transscleral cyclophotocoagulation groups, respectively (p<0.001). The median preoperative logMAR visual acuity was 0.52 ± 0.69 and 1.75 ± 1.04 in the micropulse- and “slow cook” transscleral cyclophotocoagulation groups, respectively (p<0.001). The mean visual acuity variation was -0.10 ± 0.35 and -0.074 ± 0.16 in the micropulse- and “slow cook” transscleral cyclophotocoagulation, respectively (p=0.510). Preoperatively, the mean eye drops were 3.44 ± 1.38 and 2.89 ± 0.68 drugs in the micropulse- and “slow cook” transscleral cyclophotocoagulation groups, respectively (p=0.017), but those were 2.06 ± 1.42 and 1.02 ± 1.46 at the end of the study in the slow cook” and micropulse transscleral cyclophotocoagulation groups, respectively (p<0.001). The success of criterion A was not significant between both groups. Compared with 11 eyes (17.74%) in the slow cook” transscleral cyclophotocoagulation group, 19 eyes (28.78%) in the micropulse transscleral cyclophotocoagulation group showed complete success (p=0.171). For criterion B, 28 (42.42%) and 2 eyes (3.22%) showed complete success after micropulse- and slow cook” transscleral cyclophotocoagulation, respectively (p<0.001).
CONCLUSION: Both techniques reduced intraocular pressure effectively.
Keywords: Sclera/surgery; Glaucoma, open-angle/surgery; Ciliary body/surgery; Intraocular pressure; Laser coagulation/methods; Lasers, semiconductor; Comparative study; Effectiveness
Arq. Bras. Oftalmol. 2021;84 (4 )
:361-366
| DOI: 10.5935/0004-2749.20210052
Abstract
OBJETIVO: Glaucoma é a principal causa de cegueira irreversível no mundo. O pico da pressão intraocular é um dos principais fatores de risco para progressão do glaucoma, e o controle pressórico ainda é o único tratamento efetivo para todas as formas de glaucoma. O objetivo principal deste estudo é comparar a redução basal e do pico da pressão intraocular, obtidas através do Teste de Sobrecarga Hídrica, entre os dois olhos dos mesmos pacientes utilizando latanoprosta 0,005% em um olho e submetidos à aplicação de trabeculoplastia a laser seletiva no olho contralateral.
MÉTODOS: Este é um estudo prospectivo, intervencionista, longitudinal e randomizado. Trinta pacientes consecutivos, glaucomatosos, com pressão intraocular controlada em uso de monoterapia com latanoprosta, foram recrutados de um único centro oftalmológico. Os olhos dos pacientes foram randomizados e um olho foi selecionado para tratamento com trabeculoplastia a laser seletiva e olho contralateral tratado com colírio de latanoprosta 0,005%. Foram avaliados a pressão intraocular basal e pico de pressão intraocular um mês (Teste de Sobrecarga Hídrica 2) e seis meses (Teste de Sobrecarga Hídrica 3) após tratamento.
RESULTADOS: Não houve diferença estatística entre a pressão intraocular pré washout entre os olhos randomizados para trabeculoplastia a laser seletiva e latanoprosta, 13,6 ± 2,1 e 13,3 ± 1,8 mmHg, respectivamente (p=0,182). Em relação à pressão intraocular basal, não houve diferença estatística entre os grupos, tanto no Teste de Sobrecarga Hídrica 2 (p=0,689) e Teste de Sobrecarga Hídrica 3 (p=0,06). Não houve diferença estatística em relação ao pico de pressão intraocular entre os grupos trabeculoplastia a laser seletiva e latanoprosta, no Teste de Sobrecarga Hídrica 2 (p=0,771) e Teste de Sobrecarga Hídrica 3 (p=0,774).
CONCLUSÕES: Em resumo, nosso estudo demonsrou que a eficácia da redução pressórica é similar entre latanoprosta e trabeculoplastia a laser seletiva, e pacientes glaucomatosos que estão com a pressão intraocular clinicamente controlados com latanoprosta e trocam de tratamento para trabeculoplastia a laser seletiva mantém sua pressão intraocular controlada.
Keywords: Glaucoma; Pressão intraocular; Latanoprosta; Lasers
Arq. Bras. Oftalmol. 2025;88 (6 )
:1-5
| DOI: 10.5935/0004-2749.2024-0340
Abstract
PURPOSE: This study aimed to report the surgical outcomes and success predictors of micropulse transscleral cyclophotocoagulation in eyes with refractory glaucoma.
METHODS: This was a noncomparative, interventional case series. Patients with refractory glaucomas, defined as eyes with prior incisional glaucoma surgery failure and uncontrolled intraocular pressure, who underwent micropulse transscleral cyclophotocoagulation between March 2017 and June 2021 were enrolled. A minimum follow-up period of 6 months was required. Preoperative and postoperative intraocular pressure, number of hypotensive medications, surgical complications, and any subsequent related events were recorded. Success criteria were as follows: 1) intraocular pressure reduction ≥20% and intraocular pressure ≤18 mmHg; 2) intraocular pressure reduction ≥30% and intraocular pressure ≤15 mmHg. The need for topical hypotensive medications was not considered a failure.
RESULTS: Seventy-nine (79) eyes (79 patients; mean age, 57.5 ± 20.6 years) were included. Overall, the median follow-up duration was 12.0 (interquartile interval, 6–24) months, and the mean intraocular pressure was reduced from 22.8 ± 6.8 mmHg to 15.5 ± 5.6 mmHg at the last follow-up visit (p<0.001). The mean number of medications was reduced from 2.8 ± 0.7 to 2.0 ± 1.0 (p<0.01). At 12 months postoperatively, the success rates for criteria 1 and 2 were 54.9% and 49.7%, respectively. Aside from one case of corneal ulcer, which fully resolved with clinical treatment, and two cases of persistent hypotony (with no visual acuity loss during follow-up), no other vision-threatening complications were observed during the postoperative period. The magnitude of intraocular pressure reduction at 1 month (adjusted to preoperative intraocular pressure; HR=1.01; p=0.002).
CONCLUSION: Our findings suggest that micropulse transscleral cyclophotocoagulation is a relatively effective alternative for managing refractory glaucomas, with minor postoperative complications. In addition, the initial intraocular pressure reduction was a statistically significant predictor of 1-year success in patients undergoing micropulse transscleral cyclophotocoagulation.
Keywords: Intraocular pressure/physiology; Glaucoma, open-angle/surgery; Trabeculectomy; Laser coagulation/methods; Tonometry, ocular/methods; Postoperative complications; Antihypertensive agents/therapeutic use.
Arq. Bras. Oftalmol. 2026;89 (3 )
:1-8
| DOI: 10.5935/0004-2749.2025-0043
Abstract
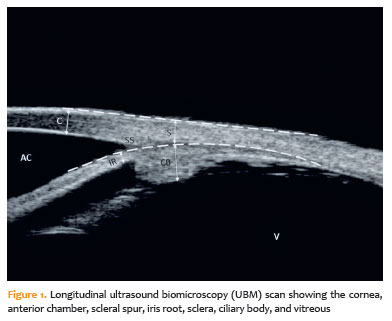
PURPOSE: To evaluate the effect of single-session transscleral diode laser cyclophotocoagulation on intraocular pressure in refractory glaucoma and to determine structural changes using ultrasound biomicroscopy.
METHODS: Forty-three eyes were evaluated. Intraocular pressures at baseline and at the first, third, and sixth months after transscleral diode laser cyclophotocoagulation were compared. Ciliary body thickness, ciliary muscle thickness, ciliary process thickness, iris root thickness, and scleral thickness were assessed at baseline and at the third and sixth months post-treatment.
RESULTS: Reductions in intraocular pressure were significant between baseline and the first month (p=0.018), third month (p<0.001), and sixth month (p<0.001) as well as between the first and third months (p=0.034) and the first and sixth months (p=0.036). Compared with baseline, intraocular pressure reduction rates at the first, third, and sixth months were 34.6%, 56.5%, and 55.3%, respectively, while success rates were 30.2%, 62.8%, and 55.8%, respectively. Decreases in ciliary body thickness, ciliary muscle thickness, and ciliary process thickness were significant between baseline and the third month (p<0.05) and between baseline and the sixth month (p<0.05), whereas changes between the third and sixth months were not significant (p>0.05). Iris root and scleral thicknesses did not change after treatment (p>0.05). At the third and sixth months, significant positive correlations were observed between changes in intraocular pressure and changes in ciliary body thickness and ciliary process thickness (p<0.05).
CONCLUSIONS: To the best of our knowledge, this is one of the few studies comprehensively investigating structural changes after transscleral diode laser cyclophotocoagulation using ultrasound biomicroscopy. Moreover, the relationships between intraocular pressure changes and variations in the ciliary body, ciliary muscle, ciliary process, iris root, and scleral thicknesses were examined in detail. Single-session treatment did not affect iris root or scleral thickness but significantly reduced ciliary body, ciliary muscle, and ciliary process thicknesses. Greater reductions in ciliary body and ciliary process thickness may contribute to more pronounced intraocular pressure reduction.
Keywords: Intraocular pressure; Laser coagulation/methods; Lasers, semiconductor; Microscopy, acoustic; Glaucoma; Ciliary body
Arq. Bras. Oftalmol. 2025;88 (2 )
:1-9
| DOI: 10.5935/0004-2749.2023-0292
Abstract
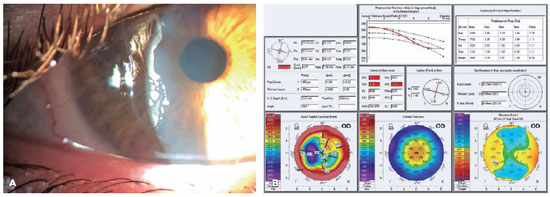
PURPOSE: Myopia, or nearsightedness, is one of the most common eye conditions worldwide. However, a comparison of the effectiveness of different laser-assisted interventions is lacking. Thus, we aimed to compare the efficacy and safety of LASIK and IntraLASIK in addressing myopia.
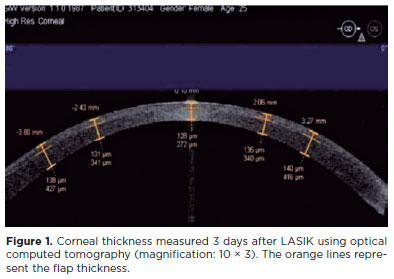
METHODS: The study was conducted in two ophthalmology clinics in Beijing, China, in 2022. A total of 84 patients (152 eyes) with different degrees of myopia were examined and underwent LASIK (n=46, 80 eyes) or IntraLASIK (n=38, 72 eyes). Keratometry, corneal topography, pachymetry, visual acuity evaluation, and corneal biomechanical analysis were performed before and after the intervention.
RESULTS: IntraLASIK produced more precise flaps than LASIK, with deviations of <8 mm and 0.1 mm from the intended thickness and diameter, respectively. LASIK resulted in nonuniform flaps, with thickness deviations of 5-86 mm. IntraLASIK demonstrated a superior efficacy for patients with severe myopia and thin corneas, with a mean spherical equivalent of 0.9 D at 6 months compared to the 1.4 D for LASIK. Approximately 91% and 83% of the patients with mild to moderate and severe myopia, respectively, achieved results within ± 0.49 D from the refractive target with IntraLASIK.
CONCLUSIONS: Corneal hysteresis and corneal resistance factor decreased with an increase in laser intensity, and they decreased faster with thinner corneas. Thus, IntraLASIK is more useful than LASIK in patients with thin corneas and severe myopia.
Keywords: Myopia; Lasers; Cornea; Keratomileusis; Laser in situ
Arq. Bras. Oftalmol. 2026;89 (3 )
:1-8
| DOI: 10.5935/0004-2749.2025-0330
Abstract
PURPOSE: To assess whether low-concentration brimonidine (0.025%) improves early postoperative signs and symptoms following femtosecond laser-assisted in situ keratomileusis and photorefractive keratectomy without affecting pupil diameter or flap safety.
METHODS: This prospective, randomized, double-masked, contralateral-eye, single-center study was conducted between January and September 2024. In each patient, one eye received 0.025% brimonidine 15–30 min before surgery (mean: 21.3 ± 2.4 min), whereas the fellow eye received 0.15% sodium hyaluronate (control). Primary outcomes on postoperative Day 1 included subconjunctival hemorrhage laser-assisted in situ keratomileusis and patient-reported symptoms (0–10 scale; composite score). Pupil diameter was measured pre-ablation. Statistical analyses included McNemar and paired t tests, with a significant threshold of α=0.05.
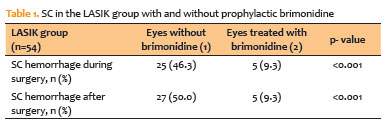
RESULTS: A total of 124 patients were included (54 laser-assisted in situ keratomileusis and 70 photorefractive keratectomy). Pupil diameter did not differ significantly between brimonidine-treated and control eyes (laser-assisted in situ keratomileusis: 2.63 ± 0.47 vs. 2.69 ± 0.42 mm, p=0.273; photorefractive keratectomy: 2.56 ± 0.44 vs. 2.61 ± 0.39 mm, p=0.116). In laser-assisted in situ keratomileusis, subconjunctival hemorrhage occurred less frequently in brimonidine-treated eyes both intraoperatively (9.3% vs. 46.3%, p<0.001) and on postoperative Day 1 (9.3% vs. 50.0%, p<0.001). Composite symptom scores were significantly lower in brimonidine-treated eyes in both laser-assisted in situ keratomileusis and photorefractive keratectomy groups (p=0.001 for both).
CONCLUSIONS: Preoperative administration of low-concentration brimonidine (0.025%) significantly reduced subconjunctival hemorrhage in laser-assisted in situ keratomileusis without comprising flap integrity. It also improved early postoperative symptoms in laser-assisted in situ keratomileusis and photorefractive keratectomy, without affecting pupil diameter. These findings support the use of dilute brimonidine as a safe and effective adjunct to enhance the immediate postoperative experience in refractive surgery.
Keywords: Brimonidine tartrate; Postoperative pain; Subconjunctival hemorrhage; Refractive surgery; Hemorrhage; Keratomileusis, laser in situ; Photorefractive keratectomy
 ABO is licensed under a Creative Commons Attribution-NonComercial 4.0 Internacional.
ABO is licensed under a Creative Commons Attribution-NonComercial 4.0 Internacional.
12-tab01tb.jpg)
08-fig01.jpg)
13-tab01tb.jpg)
09-tab01tb.jpg)

11-fig01.jpg)
01-tab01tb.jpg)
05-fig01tb.jpg)
04-fig01.jpg)