Showing of 1 until 15 from 164 result(s)
Search for: Intraocular pressure; Glaucoma surgery; Trabeculectomy; Postoperative; Mitomycin C
Abstract
Objetivo: Avaliar o sucesso na redução da pressão intra-ocular, com a utilização de trabeculectomia simples e quando associada a 5-fluorouracil ou mitomicina-C e avaliar se o tempo de exposição à mitomicina-C modifica este índice de sucesso. Métodos: Analisaram-se retrospectivamente 171 olhos consecutivos, entre janeiro de 1989 e março de 1998, sendo 16 olhos submetidos à trabeculectomia simples, 38 olhos à trabeculectomia e aplicação pós-operatória de 5-fluorouracil e 117 olhos à trabeculectomia e aplicação intra-operatória de mitomicina-C. Resultados: Os resultados mostraram uma redução significativa da PIO (pressão intra-ocular), com o uso de antifibroblásticos (p < 0,05). O tempo de exposição à mitomicina-C não apresentou diferença estatisticamente significativa (p > 0,05). Conclusões: Os autores concluem que a trabeculectomia associada a drogas antifibroblásticas reduz a PIO de maneira significativa e promove estabilidade a curto prazo.
Keywords: Trabeculectomia; 5-Fluorouracil; Mitomicina C
03-tab01.jpg)
Abstract
Objetivo: Comparar as alterações nos parâmetros do segmento anterior após a cirurgia ExPRESS Mini Glaucoma Shunt vs. trabeculectomia usando a câmera Scheimpflug Pentacam rotativa.
Métodos: Neste estudo comparativo prospectivo, 27 pacientes com glaucoma tratados no Centro Médico Rabin de 2009 a 2013 foram incluídos neste estudo comparativo prospectivo: 19 participantes (19 olhos) foram submetidos ao implante de derivação ExPRESS e 12 (13 olhos) foram submetidos à trabeculectomia. Alterações nos parâmetros da câmara anterior no dia 1 e em 3 meses de pós-operatório foram avaliadas pelas imagens de Scheimpflug.
Resultados: A pressão intraocular diminuiu significativamente em relação aos valores iniciais nos dois grupos. A diminuição nos dois grupos foi semelhante no 3º mês pós-operatório (p=0,82). A cirurgia com ExPRESS causou um aumento temporário do astigmatismo posterior da córnea (p=0,008) e uma diminuição temporária da profundidade da câmara anterior (p=0,016) e do volume (p=0,006) no primeiro dia do pós-operatório. Ao final de três meses, esses parâmetros não foram mais estatisticamente significativos (p=0,065, p=0,51 e p=0,57, respectivamente). A trabeculectomia causou um aumento temporário do astigmatismo anterior e posterior da córnea no primeiro dia do pós-operatório (p=0,003 e p=0,005, respectivamente), mas isso não foi observado ao final de 3 meses (p=1,0 e p=1,0, respectivamente). Após 3 meses, tanto o EXPRESS quanto a trabeculectomia mostraram alterações semelhantes nos parâmetros da câmara anterior.
Conclusões: O implante ExPRESS Mini para glaucoma e a trabeculectomia diminuíram significativamente a pressão intraocular e tiveram efeitos temporários nos parâmetros do segmento anterior, com pequenas diferenças entre os métodos.
Keywords: Glaucoma/cirurgia; Implantes para drenagem de glaucoma; Trabeculectomia/métodos; Pressão intraocular
Abstract
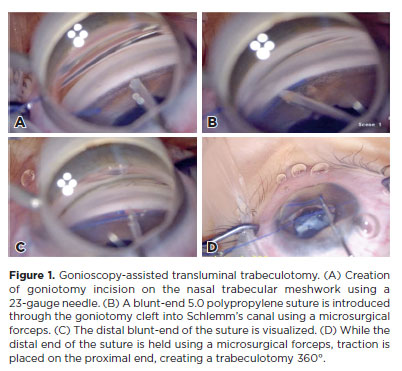
PURPOSE: To report the surgical outcomes of patients with primary congenital glaucoma who underwent gonioscopy-assisted transluminal trabeculotomy.
METHODS: This retrospective, noncomparative, interventional study included consecutive patients with primary congenital glaucoma with uncontrolled intraocular pressure undergoing gonioscopy-assisted transluminal trabeculotomy between January 2017 and January 2020. The included participants were followed up for at least 24 months, and only one surgeon performed all the procedures. The number of glaucoma medications, pre- and postoperative intraocular pressure, treatment extension (in quadrants), surgical complications, and any associated events or interventions were documented.
RESULTS: This study included 13 eyes from 10 patients (mean age, 4.5 ± 3.2 years; range, 3 months to 10 years). After a 24-month follow-up, the mean intraocular pressure significantly decreased from 26.1 ± 3.7 to 11.8 ± 2.5 mmHg (p<0.001). The mean number of glaucoma medications was reduced from 3.3 ± 0.5 to 0.85 ± 1.0 (p<0.001). At the end of the follow-up interval, all eyes (13 out of 13) had an intraocular pressure between 7 and 15 mmHg. In 11 of 13 eyes (84.6%), gonioscopy-assisted transluminal trabeculotomy was performed in all quadrants (360º). The most frequent postoperative complication was transitory (self-limited) hyphema (7 out of 13 eyes [53.8%]). No sight-threatening adverse events occurred during the entire follow-up period.
CONCLUSIONS: The 2-year follow-up results indicated gonioscopy-assisted transluminal trabeculotomy as an efficient and safe option for primary congenital glaucoma treatment with minimal postoperative complications.
Keywords: Glaucoma, Open-angle/surgery; Gonioscopy; Trabeculectomy/methods; Intraocular pressure; Antihypertensive agents/therapeutic use.
11-tab01tb.jpg)
Abstract
Objetivo: Comparar a viscotrabeculotomia com irrigação da câmara anterior com o implante de válvula de glaucoma de Ahmed para glaucoma secundário após remoção de óleo de silicone.
Métodos: Foi realizado um estudo prospectivo de 43 olhos pseudofácicos vitrectomizados com glaucoma persistente após a remoção de óleo de silicone. Os pacientes foram randomizados para viscotrabeculotomia com irrigação da câmara anterior ou implante de válvula de Ahmed. Todos os pacientes foram examinados no primeiro dia, na primeira semana e 1, 3, 6, 9, 12, 18 e 24 meses após a cirurgia. Observaram-se complicações pós-operatórias. O sucesso foi definido como uma pressão intraocular entre 6 e 20 mmHg e uma redução da pressão intraocular >30% em comparação com a pressão intraocular pré-operatória.
Resultados: Foram designados 22 olhos para o grupo da viscotrabeculotomia com irrigação da câmara anterior e 21 olhos para o grupo do implante de válvula de Ahmed. A pressão intraocular média pré-operatória foi de 35,5 ± 2,6 mmHg para o grupo da viscotrabeculotomia com irrigação da câmara anterior e pós- e de 35,5 ± 2,4 mmHg no grupo do implante de válvula de Ahmed. e Os valores pós-operatórios foram de 16,9 ± 0,7 mmHg e 17,9 ± 0,9 mmHg para esses mesmos grupos, respectivamente (p<0,0001). Ambos os grupos tiveram uma redução estatisticamente significativa da pressão intraocular em relação aos valores pré-operatórios (p<0,0001) em todos os momentos do acompanhamento. A taxa de sucesso não qualificado nos grupos da viscotrabeculotomia com irrigação da câmara anterior e do implante de válvula de Ahmed foi de 72,73% e 61,9%, respectivamente. A complicação mais comum foi o hifema, autolimitado e mínimo.
Conclusões: Tanto a viscotrabeculotomia com irrigação da câmara anterior quanto o implante de válvula de Ahmed são eficazes na redução da pressão intraocular no glaucoma após injeção de óleo de silicone, mas a viscotrabeculotomia com irrigação em câmara anterior proporcionou maior redução da pressão intraocular e maiores taxas de sucesso, com complicações mínimas.
Keywords: Implante para drenagem de glaucoma; Glaucoma; Descolamento retiniano; Óleo de silicone; Trabeculectomia; Injeção intravítrea; Pressão intraocular; Complicação pós-operatória; Solução oftálmica; Dexametasona; Ofloxacino.
Abstract
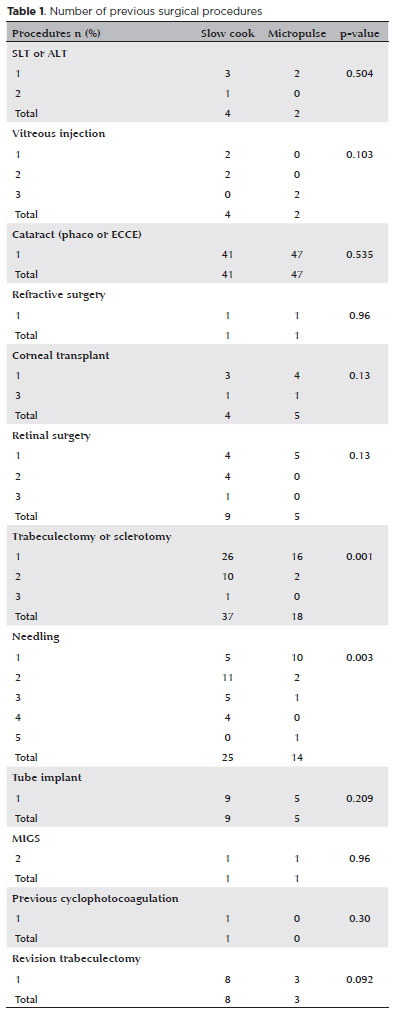
PURPOSE: This study aimed to compare the safety and effectiveness of intraocular pressure reduction between micropulse transscleral cyclophotocoagulation and “slow cook” transscleral cyclophotocoagulation in patients with refractory primary open-angle glaucoma.
METHODS: We included patients with primary open angle glaucoma with at least 12 months of follow-up. We collected and analyzed data on the preoperative characteristics and postoperative outcomes. The primary outcomes were a reduction of ≥20% of the baseline value (criterion A) and/or intraocular pressure between 6 and 21 mmHg (criterion B).
RESULTS: We included 128 eyes with primary open-angle glaucoma. The preoperative mean intraocular pressure was 25.53 ± 6.40 and 35.02 ± 12.57 mmHg in the micropulse- and “slow cook” transscleral cyclophotocoagulation groups, respectively (p<0.001). The mean intraocular pressure was reduced significantly to 14.33 ± 3.40 and 15.37 ± 5.85 mmHg in the micropulse- and “slow cook” transscleral cyclophotocoagulation groups at the last follow-up, respectively (p=0.110). The mean intraocular pressure reduction at 12 months was 11.20 ± 11.46 and 19.65 ± 13.22 mmHg in the micropulse- and “slow cook” transscleral cyclophotocoagulation groups, respectively (p<0.001). The median preoperative logMAR visual acuity was 0.52 ± 0.69 and 1.75 ± 1.04 in the micropulse- and “slow cook” transscleral cyclophotocoagulation groups, respectively (p<0.001). The mean visual acuity variation was -0.10 ± 0.35 and -0.074 ± 0.16 in the micropulse- and “slow cook” transscleral cyclophotocoagulation, respectively (p=0.510). Preoperatively, the mean eye drops were 3.44 ± 1.38 and 2.89 ± 0.68 drugs in the micropulse- and “slow cook” transscleral cyclophotocoagulation groups, respectively (p=0.017), but those were 2.06 ± 1.42 and 1.02 ± 1.46 at the end of the study in the slow cook” and micropulse transscleral cyclophotocoagulation groups, respectively (p<0.001). The success of criterion A was not significant between both groups. Compared with 11 eyes (17.74%) in the slow cook” transscleral cyclophotocoagulation group, 19 eyes (28.78%) in the micropulse transscleral cyclophotocoagulation group showed complete success (p=0.171). For criterion B, 28 (42.42%) and 2 eyes (3.22%) showed complete success after micropulse- and slow cook” transscleral cyclophotocoagulation, respectively (p<0.001).
CONCLUSION: Both techniques reduced intraocular pressure effectively.
Keywords: Sclera/surgery; Glaucoma, open-angle/surgery; Ciliary body/surgery; Intraocular pressure; Laser coagulation/methods; Lasers, semiconductor; Comparative study; Effectiveness
12-fig01tb.jpg)
Abstract
Objetivo: Descrever a frequência, as características clínicas, as complicações e o manejo do glaucoma em olhos submetidos a implantes de ceratoprótese.
Métodos: Pacientes submetidos à cirurgia de ceratoprótese entre junho de 2010 e janeiro de 2020 foram avaliados retrospectivamente em termos de glaucoma associado e prognóstico.
Resultados: Dos 17 pacientes submetidos à cirurgia de ceratoprótese, em 9 (52,9%) foi constatado glaucoma subjacente ou induzido por ceratoprótese. Cinco olhos (29,4%) tinham glaucoma subjacente e receberam a implantação de um dispositivo de drenagem de glaucoma pelo menos 6 meses antes da cirurgia de ceratoprótese. Um olho (5,9%) com pressão intraocular normal teve implantado um dispositivo de drenagem de glaucoma na mesma sessão da cirurgia de ceratoprótese, devido às características de “alto risco” das estruturas do segmento anterior. Quatro dos olhos com glaucoma preexistente apresentaram progressão após a cirurgia de ceratoprótese. Foi iniciado um tratamento antiglaucomatoso adicional em 2 olhos, enquanto outros 2 olhos receberam o implante de um segundo dispositivo de drenagem de glaucoma. Foram observadas complicações pós-operatórias em 3 olhos (100%) com dispositivo de drenagem de glaucoma implantado 6 meses antes ou na mesma sessão da cirurgia de ceratoprótese tipo afácica com vitrectomia parcial, incluindo descolamento de retina regmatogênico em 2 olhos e endoftalmite bacteriana em 1 olho. Em 1 olho observou-se migração do óleo de silicone para a área subconjuntival através do tubo após vitrectomia via pars plana. Nenhum dos 3 olhos (0%) implantados com dispositivo de drenagem de glaucoma anos antes da cirurgia de ceratoprótese apresentou complicações do segmento posterior, exceto progressão glaucomatosa. Dos 11 olhos sem história prévia de glaucoma, 3 (27,3%) apresentaram alta pressão intraocular e alterações do disco glaucomatoso após cirurgia de ceratoprótese, condições que podem ser controladas clinicamente.
Conclusões: Nesta coorte, os olhos com glaucoma pré-existente foram mais difíceis de manejar, comparados àqueles que desenvolveram glaucoma após a cirurgia de ceratoprótese. Apareceram mais complicações retinianas quando o implante do dispositivo de drenagem de glaucoma foi realizado no máximo 6 meses antes da cirurgia de ceratoprótese do tipo afácico com vitrectomia parcial.
Keywords: Glaucoma/cirurgia; Pressão intraocular; Complicação pós-operatória; Implantação de prótese; Implante para drenagem de glaucoma
10-tab01.jpg)
Abstract
Objetivo: Avaliar o efeito do tabagismo nos desfechos da trabeculectomia.
Métodos: Uma revisão retrospectiva do gráfico de pacientes com glaucoma submetidos à trabeculectomia foi realizada por um único cirurgião entre 2007 e 2016. Os gráficos foram examinados para uma história documentada de condição de fumante antes da cirurgia. Variáveis pré-operatórias clínicas e demográficas e clínicas foram registradas. Os pacientes foram divididos em dois grupos de acordo com sua história de tabagismo em fumantes e não fumantes. Quaisquer Intervenções relacionadas à bolha, por exemplo, injeções de 5-fluorouracil + lise de sutura com laser, ou revisão da bolha realizada durante o período pós-operatório foram observadas. O sucesso foi definido como pressão intraocular > 5 mmHg e < 21 mm Hg sem (sucesso completo) ou com (sucesso qualificado) medicamentos hipotensores oculares. A falha foi identificada como violação dos critérios mencionados acima.
Resultados: O estudo incluiu 98 olhos de 83 pacientes com idade média de 70,7 ± 11,09 anos, sendo 53% (44/83) dos pacientes do sexo feminino. O diagnóstico mais comum foi o glaucoma de ângulo aberto primário com 47 casos (47,9%). O Grupo de fumantes incluiu 30 olhos de 30 pacientes. Os fumantes, quando comparados aos não fumantes, apresentaram uma melhor acuidade visual pré-operatória significativamente pior (p=0,038), maior espessura central da córnea (p=0,047) e maior pressão intraocular pré-operatória (p=0,011). A taxa de sucesso de um ano para a cirurgia de trabeculectomia foi de 56,7% no Grupo de fumantes contra 79,4% no Grupo de não fumantes (p=0,020). O tabagismo apresentou razão de chances para falha de 2,95 95% de IC (1,6-7,84).
Conclusão: Os fumantes demonstraram uma taxa de sucesso significativamente menor em um ano após a trabeculectomia em comparação com os não fumantes e uma maior necessidade de intervenções relacionadas à bolha.
Keywords: Glaucoma de ângulo aberto; Trabeculectomia; Pressão intraocular; Tabagismo; Tabaco/efeitos adversos; Acuidade visual
Abstract
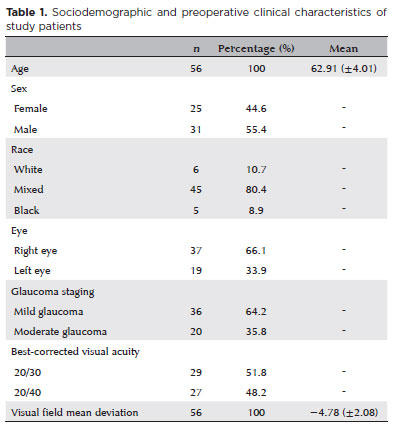
PURPOSE: Glaucoma is a chronic and progressive disease that requires long-term treatment and continuous monitoring. The Kahook Dual Blade, a device used to perform goniotomy in adults, is designed to improve intraocular pressure control in patients with glaucoma. This study aimed to evaluate the long-term efficacy and safety of kahook dual blade goniotomy in glaucoma patients undergoing cataract surgery over a 36-month follow-up.
METHODS: This was a retrospective case series including 56 eyes from 56 patients with mild-to-moderate primary open-angle glaucoma who underwent phacoemulsification combined with kahook dual blade goniotomy. Mean intraocular pressure values, number of preoperative and postoperative hypotensive eye drops, procedure survival, and complications were evaluated over 36 months. Surgical success was defined as either a reduction in intraocular pressure of ≥20% with intraocular pressure between 6 and 18 mmHg without additional medication or a reduction of ≥1 eye drop with intraocular pressure between 6 and
18 mmHg.
RESULTS: The mean preoperative intraocular pressure decreased from 15.96 ± 2,83) mmHg to 13.14 ± 2,11) mmHg at 36 months, representing a 14.9% reduction (p<0.001). The mean number of eye drops decreased from 1.91 ± 0,75) to 1.34 ± 0,92), a 29.8% reduction (p<0.001). The overall success rate was 69.6% at 36 months.
CONCLUSION: Kahook dual blade goniotomy combined with cataract surgery significantly reduced intraocular pressure and the number of hypotensive eye drops required in patients with mild-to-moderate primary open-angle glaucoma, with a favorable success rate maintained at 36 months.
Keywords: Glaucoma, open-angle/surgery; Gonioscopy/methods; Intraocular pressure/physiology; Lens implantation, intraocular; Phacoemulsification/methods; Trabeculectomy/instrumentation; Treatment outcome

Abstract
PURPOSE: This study aimed to report the surgical outcomes and success predictors of micropulse transscleral cyclophotocoagulation in eyes with refractory glaucoma.
METHODS: This was a noncomparative, interventional case series. Patients with refractory glaucomas, defined as eyes with prior incisional glaucoma surgery failure and uncontrolled intraocular pressure, who underwent micropulse transscleral cyclophotocoagulation between March 2017 and June 2021 were enrolled. A minimum follow-up period of 6 months was required. Preoperative and postoperative intraocular pressure, number of hypotensive medications, surgical complications, and any subsequent related events were recorded. Success criteria were as follows: 1) intraocular pressure reduction ≥20% and intraocular pressure ≤18 mmHg; 2) intraocular pressure reduction ≥30% and intraocular pressure ≤15 mmHg. The need for topical hypotensive medications was not considered a failure.
RESULTS: Seventy-nine (79) eyes (79 patients; mean age, 57.5 ± 20.6 years) were included. Overall, the median follow-up duration was 12.0 (interquartile interval, 6–24) months, and the mean intraocular pressure was reduced from 22.8 ± 6.8 mmHg to 15.5 ± 5.6 mmHg at the last follow-up visit (p<0.001). The mean number of medications was reduced from 2.8 ± 0.7 to 2.0 ± 1.0 (p<0.01). At 12 months postoperatively, the success rates for criteria 1 and 2 were 54.9% and 49.7%, respectively. Aside from one case of corneal ulcer, which fully resolved with clinical treatment, and two cases of persistent hypotony (with no visual acuity loss during follow-up), no other vision-threatening complications were observed during the postoperative period. The magnitude of intraocular pressure reduction at 1 month (adjusted to preoperative intraocular pressure; HR=1.01; p=0.002).
CONCLUSION: Our findings suggest that micropulse transscleral cyclophotocoagulation is a relatively effective alternative for managing refractory glaucomas, with minor postoperative complications. In addition, the initial intraocular pressure reduction was a statistically significant predictor of 1-year success in patients undergoing micropulse transscleral cyclophotocoagulation.
Keywords: Intraocular pressure/physiology; Glaucoma, open-angle/surgery; Trabeculectomy; Laser coagulation/methods; Tonometry, ocular/methods; Postoperative complications; Antihypertensive agents/therapeutic use.

Abstract
PURPOSE: This study aims to describe the technique, feasibility, efficacy, and safety of 360° trabeculotomy ab externo with double access for the treatment of congenital glaucoma.
METHODS: This paper provides a detailed description of the 360° trabeculotomy ab externo with double access used to treat pediatric glaucoma. The postoperative outcomes of six eyes from six patients who underwent this procedure for primary and secondary congenital glaucoma are also reported.
RESULTS: Six eyes from six patients were included in this study. The median age of the patients at the time of surgery was 1.25 yr (range: 0.27-5.41 yr). The mean preoperative intraocular pressure was 25 ± 5.87 mmHg (range: 18-35 mmHg). At baseline, the mean number of hypotensive eye drop medications used was 2 ± 0.63. Postoperatively, the mean intraocular pressure decreased to 10 ± 2.20 mmHg (range: 9-14 mmHg), and none of the patients required hypotensive eye drops. The most common postoperative complication was hyphema, observed in one case on the first postoperative day; however, it resolved within 7 days.
CONCLUSIONS: The 360° trabeculotomy ab externo with double access is a valuable addition to the surgical options for pediatric glaucoma. This technique facilitates a complete 360° ab externo opening of the trabecular meshwork while enhancing surgical safety.
Keywords: Glaucoma; Glaucoma/congenital; Trabeculectomy; Intraocular pressure; Ophthalmic solutions; Trabecular meshwork; Child
Abstract
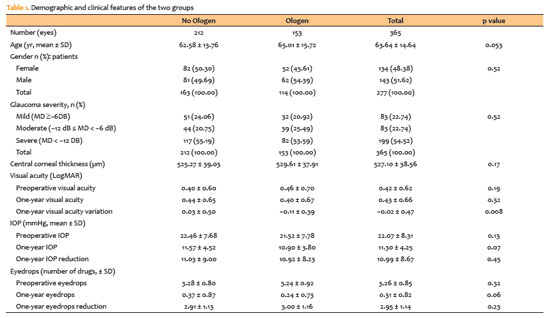
PURPOSE: To compare the efficacy and safety of trabeculectomy with mitomycin C, performed with versus without adjunctive Ologen collagen matrix in a multicenter real-world setting.
METHODS: This multicenter retrospective comparative study included 277 patients (365 eyes) who underwent trabeculectomy with mitomycin C, with or without Ologen, between 2017 and 2022 across five Brazilian centers. Extracted data comprised demographic characteristics, glaucoma subtype, intraocular pressure, number of glaucoma medications, postoperative interventions, complications, and additional surgical procedures. Surgical success was defined using two criteria: (1) intraocular pressure ≤21mmHg with ≥20% reduction from baseline and (2) final intraocular pressure between 6 and 21mmHg. Outcomes were categorized as complete (without medications) or qualified (with medications).
RESULTS: Both groups achieved substantial reductions in intraocular pressure and medication burden at 12 months, with high rates of complete and qualified success under both definitions. The Ologen group required fewer suture lysis procedures (49.0% vs. 60.8%; p=0.025), suggesting a modulatory effect on early postoperative fibrosis. Rates of other postoperative interventions, complications, and additional glaucoma surgeries were comparable between groups. Kaplan–Meier analysis demonstrated no significant difference in cumulative success over time.
CONCLUSION: Trabeculectomy with mitomycin C is effective and safe regardless of adjunctive Ologen use. Although Ologen did not confer superior long-term efficacy, its association with reduced suture lysis suggests a potential role in modulating early wound healing.
Keywords: Trabeculectomy, Intraocular pressure, Mitomycin C; Wound healing; Sutures

Abstract
PURPOSE: This study aims to compare the initial ocular discomfort symptoms resulting from trabeculectomy and Ahmed glaucoma valve implantation surgeries.
METHODS: A prospective comparative study was conducted. The evaluation of ocular discomfort employed a questionnaire designed to identify the frequency and severity of distinct symptoms: ocular pain, general discomfort, tearing, foreign body sensation, and burning. This questionnaire was administered prior to surgery as a baseline, and subsequently at 7, 30, and 90 days post-surgery. Simultaneously, the Ocular Surface Disease Index (OSDI) was applied at these same time intervals.
RESULTS: The study encompassed a total of 17 patients (9 undergoing trabeculectomy and 8 undergoing Ahmed glaucoma valve implantation). The Ahmed glaucoma valve implantation group exhibited higher tearing levels at baseline (p=0.038). However, no statistically significant differences in symptoms were observed between the two surgeries at 7 and 30 days post-surgery. At the 90-day mark following surgery, patients who had undergone trabeculectomy reported a significantly higher foreign body sensation (p=0.004). Although OSDI scores did not differ between groups at baseline, the trabeculectomy group showed significantly higher OSDI scores than the Ahmed glaucoma valve implantation group at 7, 30, and 90 days after surgery (p<0.05).
CONCLUSION: Post-surgery, patients who had undergone trabeculectomy experienced increased foreign body sensation. Trabeculectomy appears to cause greater early postoperative ocular discomfort compared to the Ahmed glaucoma valve implantation group.
Keywords: Glaucoma/surgery; Paresthesia; Trabeculectomy; Glaucoma drainage implants; Postoperative care
Abstract
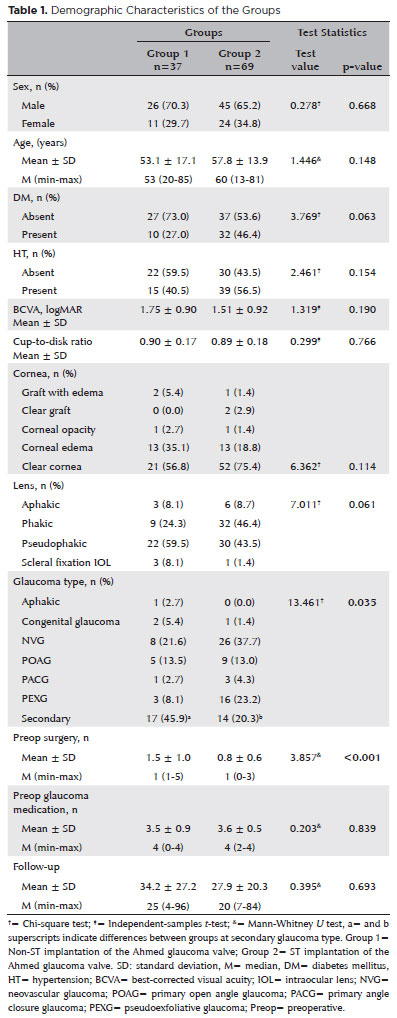
PURPOSE: As superotemporal implantation of the Ahmed glaucoma valve is not always feasible in cases of refractory glaucoma, this study examined the characteristics and surgical outcomes of cases in which the valve was implanted in a nonsuperotemporal quadrant using a modified long scleral tunnel technique.
METHODS: This retrospective case-control study included 37 eyes with nonsuperotemporal quadrant-Ahmed glaucoma valve implantation in Group 1 and 69 eyes with superotemporal Ahmed glaucoma valve implantation in Group 2. The demographic characteristics of these groups, surgical outcomes, including complications, further surgical interventions, and surgical success rates were compared. Surgical success was defined as an intraocular pressure not exceeding 21 mmHg, accompanied by a minimum reduction of 20% in intraocular pressure from the baseline without any additional intraocular pressure-lowering procedures, and the absence of light perception loss or phthisis bulbi.
RESULTS: Group 1 had significantly higher numbers of eyes with secondary glaucoma and preoperative surgical procedures than Group 2 (p<0.05). Both groups had mean preoperative intraocular pressure values, and mean intraocular pressure values at the last visit of 34.2 and 27.9 months, 35.5 ± 1.5 and 35.8 ± 1.2 mmHg, and 14.5 ± 5 and 14.9 mmHg, respectively. Although both groups had 70.2% and 75.8% as their five-year cumulative probability of success, respectively, the rates of complications, revisional surgery, and additional surgical procedures did not differ significantly (p>0.05).
CONCLUSION: The modified long scleral tunnel technique for Ahmed glaucoma valve implantation in nonsuperotemporal quadrants achieves intraocular pressure control and complication rates comparable to superotemporal implantation.
Keywords: Glaucoma/surgery; Sclera/surgery; Glaucoma drainage implant; Intraocular pressure; Tenon capsule
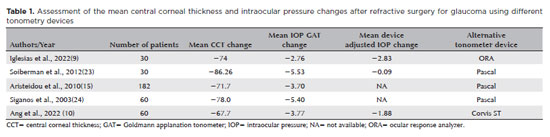
Abstract
Myopia is a significant risk factor for glaucoma and a growing public health problem worldwide. Detecting glaucomatous changes in highly myopic eyes is diagnostically challenging due to the abnormal appearance of the optic nerve head. These patients also have a greater biomechanical susceptibility to pressure-induced glaucomatous damage. Refractive surgery has become increasingly popular, and many candidates for refractive surgery are myopic. Therefore, we sought to review the aspects of patient evaluation in those who have undergone refractive surgery for myopia concerned with the detection and monitoring of glaucoma development. We identified several important elements of patient evaluation for glaucoma after refractive surgery. These included the need for both structural and functional assessments before and after surgery, and the importance of monitoring for postoperative biomechanical changes in the cornea and their impact on intraocular pressure. We conclude that, in patients who undergo refractive surgery for myopia, it is essential to assess for the presence of glaucoma, to identify staging, and to plan for long-term control of the disease, regardless of IOP.
Keywords: Glaucoma; Intraocular pressure; Myopia; Refractive surgery
Abstract
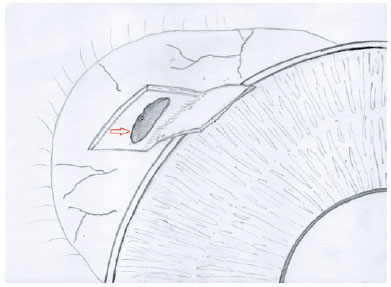
The creation of a scleral flap during trabeculectomy can be complicated by a buttonhole, partial amputation at the limbus, and extensive thinning. In some cases, the procedure must be aborted to prevent more serious postoperative complications. This report describes a technique of converting complicated trabeculectomy into ab externo cyclodialysis. A 41-year-old patient with congenital glaucoma presented with a perforated scleral wall with the choroidal tissue exposed during the dissection of the partial-thickness scleral flap. By using a Barraquer cyclodialysis spatula through the scleral perforation, the choroid was separated from the sclera up to the scleral spur over 30º into the anterior chamber. The sclera and conjunctiva/Tenon were sutured with 10-0 nylon single sutures. Two months later, the intraocular pressure was reduced to 16 mmHg with no hypotensive topical medications. This case illustrates an alternative approach to managing a flap-related perioperative complication in trabeculectomy, which yielded good early results.
Keywords: Glaucoma/surgery; Trabeculectomy; Ophthalmologic surgical procedures /adverse effects; Cyclodialisys; Postoperative complications
 ABO is licensed under a Creative Commons Attribution-NonComercial 4.0 Internacional.
ABO is licensed under a Creative Commons Attribution-NonComercial 4.0 Internacional.
About
Issues
Editorial Board
Submission
Arquivos Brasileiros de Oftalmologia
Official publication of Brazilian Council of Ophthalmology - Conselho Brasileiro de Oftalmologia (CBO)
Rua Casa do Ator, 1.117 - 2nd floor - Zip Code: 04546-004
São Paulo - SP, Brazil
TEL: +55 11 3266-4000
E-mail: [email protected]