Showing of 1 until 15 from 175 result(s)
Search for: Glaucoma; Intraocular pressure; Myopia; Refractive surgery
03-tab01.jpg)
Abstract
Objetivo: Comparar as alterações nos parâmetros do segmento anterior após a cirurgia ExPRESS Mini Glaucoma Shunt vs. trabeculectomia usando a câmera Scheimpflug Pentacam rotativa.
Métodos: Neste estudo comparativo prospectivo, 27 pacientes com glaucoma tratados no Centro Médico Rabin de 2009 a 2013 foram incluídos neste estudo comparativo prospectivo: 19 participantes (19 olhos) foram submetidos ao implante de derivação ExPRESS e 12 (13 olhos) foram submetidos à trabeculectomia. Alterações nos parâmetros da câmara anterior no dia 1 e em 3 meses de pós-operatório foram avaliadas pelas imagens de Scheimpflug.
Resultados: A pressão intraocular diminuiu significativamente em relação aos valores iniciais nos dois grupos. A diminuição nos dois grupos foi semelhante no 3º mês pós-operatório (p=0,82). A cirurgia com ExPRESS causou um aumento temporário do astigmatismo posterior da córnea (p=0,008) e uma diminuição temporária da profundidade da câmara anterior (p=0,016) e do volume (p=0,006) no primeiro dia do pós-operatório. Ao final de três meses, esses parâmetros não foram mais estatisticamente significativos (p=0,065, p=0,51 e p=0,57, respectivamente). A trabeculectomia causou um aumento temporário do astigmatismo anterior e posterior da córnea no primeiro dia do pós-operatório (p=0,003 e p=0,005, respectivamente), mas isso não foi observado ao final de 3 meses (p=1,0 e p=1,0, respectivamente). Após 3 meses, tanto o EXPRESS quanto a trabeculectomia mostraram alterações semelhantes nos parâmetros da câmara anterior.
Conclusões: O implante ExPRESS Mini para glaucoma e a trabeculectomia diminuíram significativamente a pressão intraocular e tiveram efeitos temporários nos parâmetros do segmento anterior, com pequenas diferenças entre os métodos.
Keywords: Glaucoma/cirurgia; Implantes para drenagem de glaucoma; Trabeculectomia/métodos; Pressão intraocular
Abstract
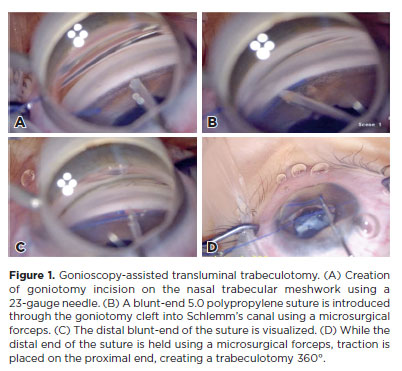
PURPOSE: To report the surgical outcomes of patients with primary congenital glaucoma who underwent gonioscopy-assisted transluminal trabeculotomy.
METHODS: This retrospective, noncomparative, interventional study included consecutive patients with primary congenital glaucoma with uncontrolled intraocular pressure undergoing gonioscopy-assisted transluminal trabeculotomy between January 2017 and January 2020. The included participants were followed up for at least 24 months, and only one surgeon performed all the procedures. The number of glaucoma medications, pre- and postoperative intraocular pressure, treatment extension (in quadrants), surgical complications, and any associated events or interventions were documented.
RESULTS: This study included 13 eyes from 10 patients (mean age, 4.5 ± 3.2 years; range, 3 months to 10 years). After a 24-month follow-up, the mean intraocular pressure significantly decreased from 26.1 ± 3.7 to 11.8 ± 2.5 mmHg (p<0.001). The mean number of glaucoma medications was reduced from 3.3 ± 0.5 to 0.85 ± 1.0 (p<0.001). At the end of the follow-up interval, all eyes (13 out of 13) had an intraocular pressure between 7 and 15 mmHg. In 11 of 13 eyes (84.6%), gonioscopy-assisted transluminal trabeculotomy was performed in all quadrants (360º). The most frequent postoperative complication was transitory (self-limited) hyphema (7 out of 13 eyes [53.8%]). No sight-threatening adverse events occurred during the entire follow-up period.
CONCLUSIONS: The 2-year follow-up results indicated gonioscopy-assisted transluminal trabeculotomy as an efficient and safe option for primary congenital glaucoma treatment with minimal postoperative complications.
Keywords: Glaucoma, Open-angle/surgery; Gonioscopy; Trabeculectomy/methods; Intraocular pressure; Antihypertensive agents/therapeutic use.
Abstract
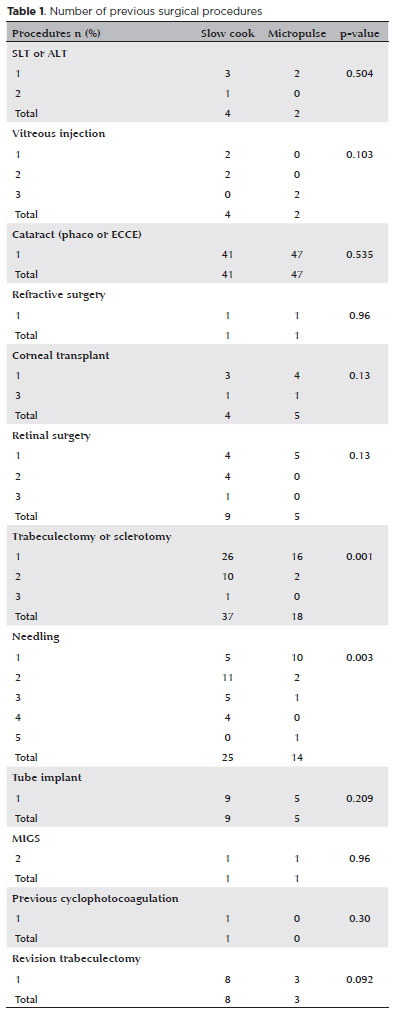
PURPOSE: This study aimed to compare the safety and effectiveness of intraocular pressure reduction between micropulse transscleral cyclophotocoagulation and “slow cook” transscleral cyclophotocoagulation in patients with refractory primary open-angle glaucoma.
METHODS: We included patients with primary open angle glaucoma with at least 12 months of follow-up. We collected and analyzed data on the preoperative characteristics and postoperative outcomes. The primary outcomes were a reduction of ≥20% of the baseline value (criterion A) and/or intraocular pressure between 6 and 21 mmHg (criterion B).
RESULTS: We included 128 eyes with primary open-angle glaucoma. The preoperative mean intraocular pressure was 25.53 ± 6.40 and 35.02 ± 12.57 mmHg in the micropulse- and “slow cook” transscleral cyclophotocoagulation groups, respectively (p<0.001). The mean intraocular pressure was reduced significantly to 14.33 ± 3.40 and 15.37 ± 5.85 mmHg in the micropulse- and “slow cook” transscleral cyclophotocoagulation groups at the last follow-up, respectively (p=0.110). The mean intraocular pressure reduction at 12 months was 11.20 ± 11.46 and 19.65 ± 13.22 mmHg in the micropulse- and “slow cook” transscleral cyclophotocoagulation groups, respectively (p<0.001). The median preoperative logMAR visual acuity was 0.52 ± 0.69 and 1.75 ± 1.04 in the micropulse- and “slow cook” transscleral cyclophotocoagulation groups, respectively (p<0.001). The mean visual acuity variation was -0.10 ± 0.35 and -0.074 ± 0.16 in the micropulse- and “slow cook” transscleral cyclophotocoagulation, respectively (p=0.510). Preoperatively, the mean eye drops were 3.44 ± 1.38 and 2.89 ± 0.68 drugs in the micropulse- and “slow cook” transscleral cyclophotocoagulation groups, respectively (p=0.017), but those were 2.06 ± 1.42 and 1.02 ± 1.46 at the end of the study in the slow cook” and micropulse transscleral cyclophotocoagulation groups, respectively (p<0.001). The success of criterion A was not significant between both groups. Compared with 11 eyes (17.74%) in the slow cook” transscleral cyclophotocoagulation group, 19 eyes (28.78%) in the micropulse transscleral cyclophotocoagulation group showed complete success (p=0.171). For criterion B, 28 (42.42%) and 2 eyes (3.22%) showed complete success after micropulse- and slow cook” transscleral cyclophotocoagulation, respectively (p<0.001).
CONCLUSION: Both techniques reduced intraocular pressure effectively.
Keywords: Sclera/surgery; Glaucoma, open-angle/surgery; Ciliary body/surgery; Intraocular pressure; Laser coagulation/methods; Lasers, semiconductor; Comparative study; Effectiveness
03-fig01.jpg)
Abstract
Objetivo: Investigar os resultados pós-operatórios e avaliar os preditores de sucesso da facoemulsificação combinada à goniotomia com o Kahook Dual Blade para o tratamento da catarata e do glaucoma em olhos com glaucoma primário de ângulo aberto.
Métodos: Série de casos retrospectivos, não comparativos e intervencionistas, em que todos os pacientes com glaucoma primário de ângulo aberto submetidos ao procedimento de facoemulsificação combinada à goniotomia com o Kahook Dual Blade entre junho de 2018 e abril de 2019 foram inscritos. Todos os participantes tiveram um acompanhamento mínimo de 6 meses. Foram registrados os valores de pressão intraocular pré e pós-operatória (em 1, 3 e 6 meses), número de medicamentos antiglaucomatosos, melhor acuidade visual corrigida, complicações cirúrgicas e quaisquer eventos ou procedimentos subsequentes relacionados. A análise de regressão logística foi usada para investigar a associação entre diferentes variáveis e resultados cirúrgicos.
Resultados: Um total de 57 olhos de 47 pacientes foram incluídos (média de idade, 70,5 ± 7 anos). A pressão intraocular média reduziu de 15,5 ± 4,2 mmHg para 12,2 ± 2,4 mmHg na última visita de acompanhamento (p<0,001). O número médio de medicamentos antiglaucomatosos diminuiu significativamente de 1,9 ± 1,0 para 0,6 ± 1,0 durante o mesmo período (p<0,001). Com base no critério predefinido (redução da pressão intraocular ≥20% e/ou redução de ≥1 medicamento), a taxa de sucesso em 6 meses foi de 86%. Um valor de pressão intraocular pré-operatório mais alto (OR= 2,01; p=0,016) e maior porcentagem de redução da pressão intraocular inicial
(30 dias) (OR= 1,02; p=0,033) foram significativamente associados ao sucesso cirúrgico.
Conclusão: Nossos resultados sugerem que o procedimento de facoemulsificação combinada à goniotomia com o Kahook Dual Blade é uma alternativa eficaz e segura para o manejo da catarata em olhos com glaucoma primário de ângulo aberto, impactando positivamente no controle da pressão intraocular e no número de medicamentos. Olhos com pressão intraocular basal mais alta e resposta inicial mais pronunciada ao procedimento parecem apresentar melhores resultados em 6 meses. Mais estudos são necessários para avaliar a eficácia em longo prazo e o perfil de segurança.
Keywords: Glaucoma; Glaucoma de ângulo aberto; Catarata; Facoemulsificação; Pressão intraocular; Goniotomia
12-fig01tb.jpg)
Abstract
Objetivo: Descrever a frequência, as características clínicas, as complicações e o manejo do glaucoma em olhos submetidos a implantes de ceratoprótese.
Métodos: Pacientes submetidos à cirurgia de ceratoprótese entre junho de 2010 e janeiro de 2020 foram avaliados retrospectivamente em termos de glaucoma associado e prognóstico.
Resultados: Dos 17 pacientes submetidos à cirurgia de ceratoprótese, em 9 (52,9%) foi constatado glaucoma subjacente ou induzido por ceratoprótese. Cinco olhos (29,4%) tinham glaucoma subjacente e receberam a implantação de um dispositivo de drenagem de glaucoma pelo menos 6 meses antes da cirurgia de ceratoprótese. Um olho (5,9%) com pressão intraocular normal teve implantado um dispositivo de drenagem de glaucoma na mesma sessão da cirurgia de ceratoprótese, devido às características de “alto risco” das estruturas do segmento anterior. Quatro dos olhos com glaucoma preexistente apresentaram progressão após a cirurgia de ceratoprótese. Foi iniciado um tratamento antiglaucomatoso adicional em 2 olhos, enquanto outros 2 olhos receberam o implante de um segundo dispositivo de drenagem de glaucoma. Foram observadas complicações pós-operatórias em 3 olhos (100%) com dispositivo de drenagem de glaucoma implantado 6 meses antes ou na mesma sessão da cirurgia de ceratoprótese tipo afácica com vitrectomia parcial, incluindo descolamento de retina regmatogênico em 2 olhos e endoftalmite bacteriana em 1 olho. Em 1 olho observou-se migração do óleo de silicone para a área subconjuntival através do tubo após vitrectomia via pars plana. Nenhum dos 3 olhos (0%) implantados com dispositivo de drenagem de glaucoma anos antes da cirurgia de ceratoprótese apresentou complicações do segmento posterior, exceto progressão glaucomatosa. Dos 11 olhos sem história prévia de glaucoma, 3 (27,3%) apresentaram alta pressão intraocular e alterações do disco glaucomatoso após cirurgia de ceratoprótese, condições que podem ser controladas clinicamente.
Conclusões: Nesta coorte, os olhos com glaucoma pré-existente foram mais difíceis de manejar, comparados àqueles que desenvolveram glaucoma após a cirurgia de ceratoprótese. Apareceram mais complicações retinianas quando o implante do dispositivo de drenagem de glaucoma foi realizado no máximo 6 meses antes da cirurgia de ceratoprótese do tipo afácico com vitrectomia parcial.
Keywords: Glaucoma/cirurgia; Pressão intraocular; Complicação pós-operatória; Implantação de prótese; Implante para drenagem de glaucoma
Abstract
PURPOSE: Glaucoma is one of the leading causes of irreversible blindness worldwide. When topical hypotensive agents or laser trabeculoplasty fail to adequately control the disease, escalation of therapy becomes necessary, with transscleral cyclophotocoagulation being one of the available options. Several variations of transscleral cyclophotocoagulation exist, including traditional continuous wave, MicroPulse, and slow-coagulation techniques. We propose a novel variation – custom slow-coagulation transscleral cyclophotocoagulation – which combines elements of both continuous wave and slow-coagulation approaches. This study aimed to evaluate the outcomes of this technique in patients with refractory glaucoma.
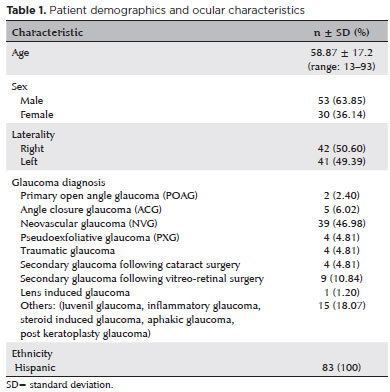
METHODS: This retrospective, interventional study included 104 eyes of 83 patients with refractory glaucoma who underwent custom slow-coagulation transscleral cyclophotocoagulation. Changes in intraocular pressure, visual acuity, the number of glaucoma medications, and postoperative complications were analyzed. A paired t test was used to compare changes in intraocular pressure and visual acuity, while the Wilcoxon signed-rank test was applied to categorical variables. Success rates following custom slow-coagulation transscleral cyclophotocoagulation were estimated using Kaplan–Meier survival analysis.
RESULTS: Mean intraocular pressure decreased significantly from 38.9 ± 15.8 mmHg at baseline to 16.3 ± 9.9 mmHg at Month 12 (p<0.001). The mean number of glaucoma medications also decreased significantly from 3.6 ± 0.6 to 1.8 ± 1.4 (p<0.001). No significant reduction in mean visual acuity was observed during follow-up.
CONCLUSIONS: Custom slow-coagulation transscleral cyclophotocoagulation effectively reduced baseline intraocular pressure and the number of glaucoma medications, with a low rate of complications and no decline in visual acuity over a 12-month follow-up period. This novel technique demonstrated a high safety profile in a Hispanic population and represents a low-cost, minimally invasive procedure with rapid recovery and promising efficacy in intraocular pressure control.
Keywords: Glaucoma/surgery; Sclera; Filtering surgery; Laser coagulation/methods; Lasers, semiconductor/therapeutic use; Intraocular pressure; Blindness/prevention & control; Vision, low/epidemiology; Visual acuity
07-fig01.jpg)
Abstract
Objetivo: Utilizar aprendizado de máquina para predizer o risco de picos de pressão intraocular às 6 AM em pacientes com glaucoma primário de ângulo aberto e suspeitos.
Métodos: Esse estudo observacional transversal incluiu 98 olhos de 98 pacientes submetidos à curva de 24 horas de pressão intraocular (incluindo as medidas às 6 AM). A curva diurna de pressão intraocular foi definida como uma série de três medidas da curva de 24 horas de pressão intraocular às 8 AM, às 9 AM e às 11 AM. Duas novas variáveis foram apresentadas: inclinação e concavidade. A inclinação da curva às 8 AM foi calculada como a diferença entre pressão intraocular às 9 AM e 8 AM e reflete a variação da pressão intraocular na primeira hora. A concavidade da curva foi calculada como a diferença entre as inclinações às 9 AM e às 8 AM e pode ser para cima ou para baixo. Uma árvore de classificação foi usada para determinar um algoritmo multivariado a partir das medidas da curva diurna para prever o risco de pressão intraocular elevada às 6 AM.
Resultados: Quarenta e nove (50%) olhos apresentaram pressão intraocular às 6 AM >21 mmHg e a mediana do pico de pressão intraocularPIO foi 26 mmHg. Os melhores preditores de pressão intraocular às 6 AM >21 mmHg foram a pressão intraocular às 8 AM e a concavidade. O modelo proposto apresentou uma sensibilidade de 100% e uma especificidade de 86%, com uma acurácia de 93%.
Conclusões: A abordagem de aprendizado de máquina foi capaz de prever o risco de picos de pressão intraocular às 6 AM com uma boa acurácia. Essa nova abordagem para a curva diurna de pressão intraocular pode se tornar uma ferramenta amplamente utilizada na prática clínica e a indicação da curva de 24 horas de pressão intraocular pode ser racionalizada de acordo com a estratificação de risco.
Keywords: Glaucoma; Glaucoma de ângulo aberto; Suspeita de glaucoma; Pressão intraocular; Aprendizado de máquina
09-tab01tb.jpg)
Abstract
OBJETIVO: Glaucoma é a principal causa de cegueira irreversível no mundo. O pico da pressão intraocular é um dos principais fatores de risco para progressão do glaucoma, e o controle pressórico ainda é o único tratamento efetivo para todas as formas de glaucoma. O objetivo principal deste estudo é comparar a redução basal e do pico da pressão intraocular, obtidas através do Teste de Sobrecarga Hídrica, entre os dois olhos dos mesmos pacientes utilizando latanoprosta 0,005% em um olho e submetidos à aplicação de trabeculoplastia a laser seletiva no olho contralateral.
MÉTODOS: Este é um estudo prospectivo, intervencionista, longitudinal e randomizado. Trinta pacientes consecutivos, glaucomatosos, com pressão intraocular controlada em uso de monoterapia com latanoprosta, foram recrutados de um único centro oftalmológico. Os olhos dos pacientes foram randomizados e um olho foi selecionado para tratamento com trabeculoplastia a laser seletiva e olho contralateral tratado com colírio de latanoprosta 0,005%. Foram avaliados a pressão intraocular basal e pico de pressão intraocular um mês (Teste de Sobrecarga Hídrica 2) e seis meses (Teste de Sobrecarga Hídrica 3) após tratamento.
RESULTADOS: Não houve diferença estatística entre a pressão intraocular pré washout entre os olhos randomizados para trabeculoplastia a laser seletiva e latanoprosta, 13,6 ± 2,1 e 13,3 ± 1,8 mmHg, respectivamente (p=0,182). Em relação à pressão intraocular basal, não houve diferença estatística entre os grupos, tanto no Teste de Sobrecarga Hídrica 2 (p=0,689) e Teste de Sobrecarga Hídrica 3 (p=0,06). Não houve diferença estatística em relação ao pico de pressão intraocular entre os grupos trabeculoplastia a laser seletiva e latanoprosta, no Teste de Sobrecarga Hídrica 2 (p=0,771) e Teste de Sobrecarga Hídrica 3 (p=0,774).
CONCLUSÕES: Em resumo, nosso estudo demonsrou que a eficácia da redução pressórica é similar entre latanoprosta e trabeculoplastia a laser seletiva, e pacientes glaucomatosos que estão com a pressão intraocular clinicamente controlados com latanoprosta e trocam de tratamento para trabeculoplastia a laser seletiva mantém sua pressão intraocular controlada.
Keywords: Glaucoma; Pressão intraocular; Latanoprosta; Lasers
Abstract
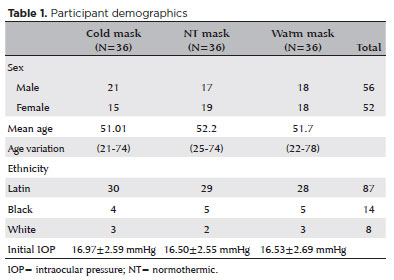
PURPOSE: This study aimed to determine whether early-stage intraocular pressure can be modulated using a thermal face mask.
METHODS:In this prospective clinical study, healthy participants were randomized on a 1:1:1 allocation ratio to three mask groups: hypothermic (G1), normothermic (G2), and hyperthermic (G3). After randomization, 108 eyes from 108 participants were submitted to clinical evaluations, including measurement of initial intraocular pressure (T1). The thermal mask was then applied for 10 minutes, followed by a second evaluation of intraocular pressure (T2) and assessment of any side effects.
RESULTS:The hypothermic group (G1) showed a significant reduction in mean intraocular pressure between T1 (16.97 ± 2.59 mmHg) and T2 (14.97 ± 2.44 mmHg) (p<0.001). G2 showed no significant pressure difference between T1 (16.50 ± 2.55 mmHg) and T2 (17.00 ± 2.29 mmHg) (p=0.054). G3 showed a significant increase in pressure from T1 (16.53 ± 2.69 mmHg) to T2 (18.58 ± 2.95 mmHg) (p<0.001). At T1, there was no difference between the three study groups (p=0.823), but at T2, the mean values of G3 were significantly higher than those of G1 and G2 (p<0.00).
CONCLUSION:Temperature was shown to significantly modify intraocular pressure. Thermal masks allow the application of temperature in a controlled, reproducible manner. Further studies are needed to assess the duration of these effects and whether they are reproducible in patients with pathologies that affect intraocular pressure.
Keywords: Intraocular pressure; Temperature; Masks; Glaucoma; Eye diseases
Abstract
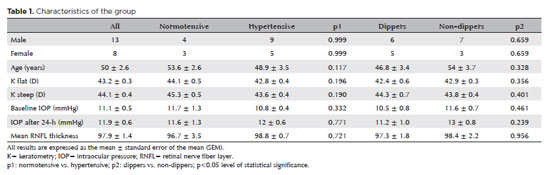
PURPOSE: This study investigated the relationship between blood pressure and intraocular pressure in treatment-naive, non-glaucoma patients with different blood pressure statuses, focusing on the 24-h ocular volume and nocturnal blood pressure decline.
METHODS: Treatment-naive, non-glaucoma patients undergoing hypertension evaluation were enrolled as study participants. Simultaneous 24-h ambulatory blood pressure measurement and 24-h ocular volume recording with a contact lens sensor. We also compared ocular volume curve parameters between normotensive and hypertensive patients, as well as between those with and without nocturnal blood pressure decline.
RESULTS: A total of 21 patients, including 7 normotensive and 14 treatment-naive hypertensive individuals, were included in the study. of them, 11 were dippers and 10 were non-dippers. No significant difference in the 24-h ocular volume slope was observed between the hypertensive and normotensive patients (p=0.284). However, dippers had a significantly higher 24-h ocular volume slope (p=0.004) and nocturnal contact lens sensor output (p=0.041) than non-dippers.
CONCLUSION: Nocturnal blood pressure decline, rather than the blood pressure level, is associated with the increased 24-h ocular volume slope and nocturnal ocular volume. Further studies are required to determine whether the acceleration of glaucoma progression in dippers is primarily due to low blood pressure, high intraocular pressure, or a combination of both.
Keywords: Intraocular pressure; Blood pressure; Contact lens; Glaucoma; Hypertension; Hypotension
Abstract
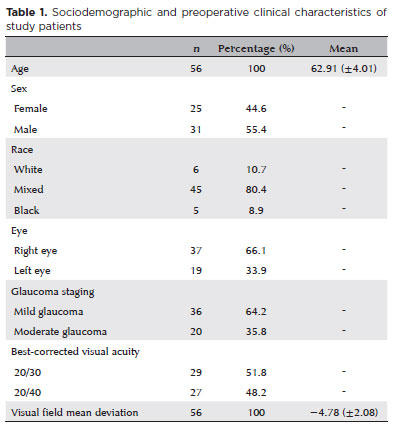
PURPOSE: Glaucoma is a chronic and progressive disease that requires long-term treatment and continuous monitoring. The Kahook Dual Blade, a device used to perform goniotomy in adults, is designed to improve intraocular pressure control in patients with glaucoma. This study aimed to evaluate the long-term efficacy and safety of kahook dual blade goniotomy in glaucoma patients undergoing cataract surgery over a 36-month follow-up.
METHODS: This was a retrospective case series including 56 eyes from 56 patients with mild-to-moderate primary open-angle glaucoma who underwent phacoemulsification combined with kahook dual blade goniotomy. Mean intraocular pressure values, number of preoperative and postoperative hypotensive eye drops, procedure survival, and complications were evaluated over 36 months. Surgical success was defined as either a reduction in intraocular pressure of ≥20% with intraocular pressure between 6 and 18 mmHg without additional medication or a reduction of ≥1 eye drop with intraocular pressure between 6 and
18 mmHg.
RESULTS: The mean preoperative intraocular pressure decreased from 15.96 ± 2,83) mmHg to 13.14 ± 2,11) mmHg at 36 months, representing a 14.9% reduction (p<0.001). The mean number of eye drops decreased from 1.91 ± 0,75) to 1.34 ± 0,92), a 29.8% reduction (p<0.001). The overall success rate was 69.6% at 36 months.
CONCLUSION: Kahook dual blade goniotomy combined with cataract surgery significantly reduced intraocular pressure and the number of hypotensive eye drops required in patients with mild-to-moderate primary open-angle glaucoma, with a favorable success rate maintained at 36 months.
Keywords: Glaucoma, open-angle/surgery; Gonioscopy/methods; Intraocular pressure/physiology; Lens implantation, intraocular; Phacoemulsification/methods; Trabeculectomy/instrumentation; Treatment outcome

Abstract
PURPOSE: This study aimed to report the surgical outcomes and success predictors of micropulse transscleral cyclophotocoagulation in eyes with refractory glaucoma.
METHODS: This was a noncomparative, interventional case series. Patients with refractory glaucomas, defined as eyes with prior incisional glaucoma surgery failure and uncontrolled intraocular pressure, who underwent micropulse transscleral cyclophotocoagulation between March 2017 and June 2021 were enrolled. A minimum follow-up period of 6 months was required. Preoperative and postoperative intraocular pressure, number of hypotensive medications, surgical complications, and any subsequent related events were recorded. Success criteria were as follows: 1) intraocular pressure reduction ≥20% and intraocular pressure ≤18 mmHg; 2) intraocular pressure reduction ≥30% and intraocular pressure ≤15 mmHg. The need for topical hypotensive medications was not considered a failure.
RESULTS: Seventy-nine (79) eyes (79 patients; mean age, 57.5 ± 20.6 years) were included. Overall, the median follow-up duration was 12.0 (interquartile interval, 6–24) months, and the mean intraocular pressure was reduced from 22.8 ± 6.8 mmHg to 15.5 ± 5.6 mmHg at the last follow-up visit (p<0.001). The mean number of medications was reduced from 2.8 ± 0.7 to 2.0 ± 1.0 (p<0.01). At 12 months postoperatively, the success rates for criteria 1 and 2 were 54.9% and 49.7%, respectively. Aside from one case of corneal ulcer, which fully resolved with clinical treatment, and two cases of persistent hypotony (with no visual acuity loss during follow-up), no other vision-threatening complications were observed during the postoperative period. The magnitude of intraocular pressure reduction at 1 month (adjusted to preoperative intraocular pressure; HR=1.01; p=0.002).
CONCLUSION: Our findings suggest that micropulse transscleral cyclophotocoagulation is a relatively effective alternative for managing refractory glaucomas, with minor postoperative complications. In addition, the initial intraocular pressure reduction was a statistically significant predictor of 1-year success in patients undergoing micropulse transscleral cyclophotocoagulation.
Keywords: Intraocular pressure/physiology; Glaucoma, open-angle/surgery; Trabeculectomy; Laser coagulation/methods; Tonometry, ocular/methods; Postoperative complications; Antihypertensive agents/therapeutic use.
11-tab01.jpg)
Abstract
Objetivo: Avaliar a influência das alterações da pressão atmosférica no comportamento da pressão intraocular de indivíduos militares saudáveis-alunos e instrutores da Escola de Mergulho e Resgate da Marinha Nacional na base naval “ARC BOLÍVAR”-durante uma imersão simulada na câmara hiperbárica do Hospital da Marinha de Cartagena.
Métodos: Realizamos um estudo exploratório descritivo. A pressão intraocular foi medida em diferentes pressões atmosféricas durante sessões de 60 minutos na câmara hiperbárica respirando ar comprimido. A profundidade máxima simulada foi de 60 pés. Os participantes eram alunos e instrutores do Departamento de Mergulho e Resgate da Base Naval.
Resultados: Quarenta e oito olhos de 24 mergulhadores foram estudados. Vinte e dois participantes (91,7%) eram do sexo masculino. A média de idade dos participantes foi de 30,6 (DP=5,5) anos, variando de 23 a 40. Nenhum participante tinha histórico de glaucoma ou hipertensão ocular. A média de base da pressão intraocular ao nível do mar foi de 14 mmHg, diminuindo para 13,1 mmHg (queda de 1,2 mmHg) a 60 pés de profundidade (p=0,0012). Entretanto, durante a parada de segurança a 30 pés, a pressão intraocular média continuou diminuindo até atingir 11,9 mmHg (p<0,001). Ao final da sessão, a pressão intraocular média atingiu 13,1 mmHg, valor inferior e estatisticamente significativo quando comparada à média de base da pressão intraocular (p=0,012).
Conclusões: Em indivíduos saudáveis, a pressão intraocular diminui ao atingir uma profundidade de 60 pés (2,8 de pressão atmosférica absoluta) e diminui ainda mais durante a ascensão a 30 pés. As medidas em ambos os pontos foram significativamente diferentes quando comparadas à pressão intraocular de base. A pressão intraocular final foi menor do que a pressão intraocular de base, sugerindo um efeito residual e prolongado da pressão atmosférica sobre a pressão intraocular.
Keywords: Pressão atmosférica; Tanometria; Pressão intraocular; Hipertensão ocular; Glaucoma; Militares
Abstract
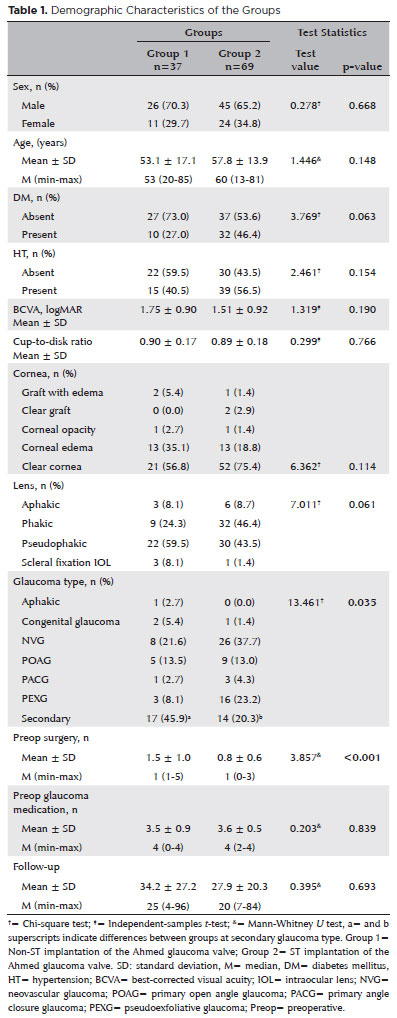
PURPOSE: As superotemporal implantation of the Ahmed glaucoma valve is not always feasible in cases of refractory glaucoma, this study examined the characteristics and surgical outcomes of cases in which the valve was implanted in a nonsuperotemporal quadrant using a modified long scleral tunnel technique.
METHODS: This retrospective case-control study included 37 eyes with nonsuperotemporal quadrant-Ahmed glaucoma valve implantation in Group 1 and 69 eyes with superotemporal Ahmed glaucoma valve implantation in Group 2. The demographic characteristics of these groups, surgical outcomes, including complications, further surgical interventions, and surgical success rates were compared. Surgical success was defined as an intraocular pressure not exceeding 21 mmHg, accompanied by a minimum reduction of 20% in intraocular pressure from the baseline without any additional intraocular pressure-lowering procedures, and the absence of light perception loss or phthisis bulbi.
RESULTS: Group 1 had significantly higher numbers of eyes with secondary glaucoma and preoperative surgical procedures than Group 2 (p<0.05). Both groups had mean preoperative intraocular pressure values, and mean intraocular pressure values at the last visit of 34.2 and 27.9 months, 35.5 ± 1.5 and 35.8 ± 1.2 mmHg, and 14.5 ± 5 and 14.9 mmHg, respectively. Although both groups had 70.2% and 75.8% as their five-year cumulative probability of success, respectively, the rates of complications, revisional surgery, and additional surgical procedures did not differ significantly (p>0.05).
CONCLUSION: The modified long scleral tunnel technique for Ahmed glaucoma valve implantation in nonsuperotemporal quadrants achieves intraocular pressure control and complication rates comparable to superotemporal implantation.
Keywords: Glaucoma/surgery; Sclera/surgery; Glaucoma drainage implant; Intraocular pressure; Tenon capsule
Abstract
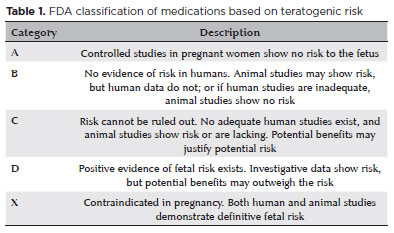
Glaucoma is a progressive optic neuropathy that can cause irreversible blindness, though it rarely affects women of reproductive age. Its management during pregnancy and lactation is particularly challenging because of the potential impact of intraocular pressure fluctuations on disease progression and the risks of treatment to both the mother and fetus. Physiological changes in pregnancy, such as decreased intraocular pressure and hormonal alterations, may influence disease activity but do not guarantee disease stability. Preconception counseling plays a key role in mitigating risks and tailoring treatment strategies. Many glaucoma medications carry teratogenic risks, with brimonidine being the only US Food and Drug Administration Category B drug. Surgical interventions – including laser trabeculoplasty and minimally invasive glaucoma surgeries – offer alternative options but require careful timing and consideration of fetal safety. Multidisciplinary collaboration is essential to optimize maternal and neonatal outcomes. This review summarizes evidence-based approaches for glaucoma management during pregnancy and lactation, highlighting clinical considerations, therapeutic strategies, and patient-centered care.
Keywords: Pregnancy complications; Glaucoma; Lactation; Parturition; Intraocular pressure
 ABO is licensed under a Creative Commons Attribution-NonComercial 4.0 Internacional.
ABO is licensed under a Creative Commons Attribution-NonComercial 4.0 Internacional.
About
Issues
Editorial Board
Submission
Arquivos Brasileiros de Oftalmologia
Official publication of Brazilian Council of Ophthalmology - Conselho Brasileiro de Oftalmologia (CBO)
Rua Casa do Ator, 1.117 - 2nd floor - Zip Code: 04546-004
São Paulo - SP, Brazil
TEL: +55 11 3266-4000
E-mail: [email protected]