Arq. Bras. Oftalmol. 2025; 88 (6): 10.5935/0004-2749.2025-0006
Total: 941
Alicia Galindo-Ferreiro1; Elvira Martinez-Fernandez1; Carolina Pereira Bigheti2,; Denise Cassia Moreira Zornoff3; Hortensia Sanchez-Tocino1; Silvana Artioli Schellini2
DOI: 10.5935/0004-2749.2025-0006
ABSTRACT
PURPOSE: This study aimed to evaluate the practices employed by oculoplastic surgeons in the assessment and management of anophthalmic sockets and external ocular prostheses.
METHODS: Oculoplastic surgeons from two countries, who specialized in the management of anophthalmic sockets, participated in a web-based survey. Data collected included demographics, types of surgery, implant use, external ocular prostheses management (including fabrication and cleaning), complications encountered, and follow-up times. The frequencies and distributions of the responses were statistically analyzed.
RESULTS: A total of 177 oculoplastic surgeons participated, 113 (63.8%) from Brazil, the remainder from Spain. Evisceration was the preferred surgical procedure of 149 (84.2%) surgeons. The most commonly reported indication for enucleation was a painful blind eye (n=103, 58.1%; both Brazil and Spain, p<0.001). Brazilian surgeons preferred polymethyl methacrylate implants (n=65, 57.5%), while Spanish surgeons favored porous polyethylene implants (n=53, 82.8%; p<0.001). Discharge was the most frequently observed clinical feature during socket evaluation (n=164, 92.6%; p<0.001). Brazilian surgeons recommended daily (n=53, 46.9%) or weekly (n=41, 36.2%) cleaning of external ocular prostheses, while Spanish surgeons more commonly recommended monthly cleaning (n=31, 48.4%; p<0.001). The majority of Brazilian surgeons (n=83, 73.4%) advised patients to remove their external ocular prostheses at night. Only a small number of Spanish surgeons (n=3, 4.6%) suggested this practice (p<0.001). Overall, the follow-up recommendations varied, with 70 (39.5%) surgeons recommending follow-up based on individual case needs, and 59 (33.3%) suggesting annual visits (p<0.001). The primary indications for external ocular prostheses replacement were edge damage (n=75, 42.3%) and loss of volume (n=68, 38.4%). The replacement intervals given typically ranged from 1 to 5 years (n=92, 51.9%; p<0.001).
CONCLUSION: Oculoplastic surgeons in Brazil and Spain demonstrated similar practices in the management of anophthalmic sockets. However, notable differences were observed in the choice of implant materials, cleaning protocols, and recommendations regarding external ocular prostheses removal during sleep.
Keywords: Anophthalmos; Eye, artificial; Polymethyl methacrylate; Polyethylene; Surgeons; Surveys and questionnaires; Brazil; Spain.
INTRODUCTION
An anophthalmic socket is a well-defined clinical condition. Combining orbital implants with external ocular prostheses (EOP) in patients with this condition is a well-established means of improving aesthetic outcomes(1). However, there is a notable gap in the literature regarding the ongoing management of these patients. Anophthalmic patients are typically managed by oculoplastic surgeons in collaboration with ophthalmologists, and EOP cleaning is generally performed by the patient under their supervision(1,2).
Care providers are tasked with providing clear and precise instructions on the appropriate care of both the prosthesis and conditions of the socket associated with anophthalmia. However, there is currently no consensus or standardized protocol regarding these care practices, particularly concerning the cleaning and handling of EOPS, and follow-up visits(2,3). Additionally, communication between healthcare professionals and patients is often suboptimal(3).
This study aims to evaluate professional practices in the routine examination, care, and management of anophthalmic sockets with EOP, as conducted by oculoplastic surgeons in Brazil and Spain. The study explores the underlying causes of anophthalmia and the preferred surgical techniques and orbital implants among oculoplastic surgeons. The findings may serve as a valuable resource, enhancing the management of patients with anophthalmic sockets.
METHODS
This qualitative, web-based study was conducted between September and December 2021. Participants were oculoplastic surgeons with expertise in anophthalmic socket management, practicing in Brazil or Spain. We aimed to evaluate the profile of patients with anophthalmic sockets, and the treatment approaches and management practices among the participants when dealing with anophthalmic sockets and EOPs. The study adhered to the principles of the 1964 Declaration of Helsinki and its later amendments. It received ethical approval from the Ethics Committee of UNESP–Botucatu Medical School (approval no. 18.618-970) and the Ethics Committee of the Rio Hortega University Hospital (approval no. PI259-20).
Participants were identified through professional medical societies, social media platforms, and general web searches. They were invited to participate via emails sent to their institutional addresses. The invitation detailed the purpose of the study and provided a link to an electronic questionnaire available in Portuguese(4) or Spanish(5). A follow-up email was sent two weeks later to improve response rates.
The questionnaire was developed by the authors and comprised 27 questions, open-ended, dichotomous and multiple-choice questions in the official language of each country. It was designed using adaptive logic, enabling the display of follow-up questions or comment boxes based on previous responses. REDCap (Research Electronic Data Capture) and Google Forms© (Google LLC, Alphabet Inc., 2021) were utilized in the design and dissemination of the survey.
All primary questions were mandatory. Some required a single response, while others allowed multiple selections, yielding a variable number of total responses. The questionnaire gathered information on the respondents’ demographics, their clinical experience with anophthalmic sockets, surgical preferences, use of orbital implants, postoperative outcomes, EOP management practices, observed complications in anophthalmic sockets, complications associated with EOPs during follow-up, and follow-up frequency.
The study responses were returned anonymously. However, the country of origin of each participant was recorded to enable comparative analysis between Brazilian and Spanish respondents. To ensure respondent anonymity, a unique numerical identifier was automatically assigned to each internet-connected device at the time of data submission.
Statistical analysis
Data were compiled in Microsoft Excel (Microsoft Corp., Redmond, WA, USA) and analyzed using frequency distributions and percentages. Non-parametric statistical tests and the chi-square test were applied to assess statistical significance (p value <0.05).
RESULTS
The questionnaire was distributed to 709 ophthalmologists–379 in Brazil and 330 in Spain. A total of 177 (25%) oculoplastic specialists responded, of whom 113 (63.8%) were from Brazil. The majority of respondents (n=140, 79%) had completed their medical training after the year 2000 and reported a high level of experience in the management of anophthalmic sockets.
Evisceration was the most commonly performed surgical technique (n=149, 84.2%). Respondents from Brazil reported limited availability of orbital implants and prostheses, with 63 (55.8%) indicating that such resources were not provided through the public healthcare system, and 52 (46.4%) stating that they were not covered by private health insurance. In contrast, all Spanish participants reported that implants and prostheses were publicly provided.
Clinical and surgical approaches
The most frequently cited indication for eye removal was a painful blind eye (n=103, 58.1%). This was a statistically significant finding in both Brazil (p<0.001) and Spain (p=0.003). The next most common reasons were phthisis bulbi (n=49, 27.6%) and ocular trauma (n=20, 11.2%). The frequencies of all causes are shown in table 1.
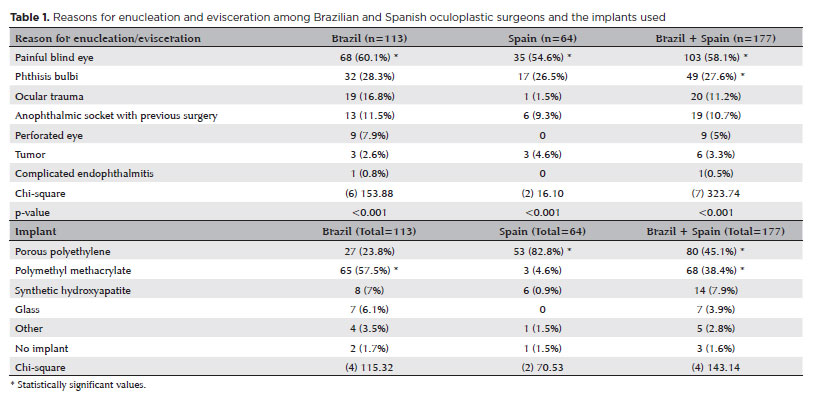
Spherical orbital implants were the most commonly utilized, as reported by 88.4% of Brazilian and 89% of Spanish surgeons. Brazilian respondents showed a preference for polymethyl methacrylate (PMMA) implants (n=65, 57.5%), whereas Spanish specialists favored porous polyethylene (PP) implants (n=53, 82.8%). This was a statistically significant difference (p<0.001) (Tables 1 and 2).

Discharge around the prosthetic eye was the most frequently observed complication in anophthalmic socket evaluations (n=164, 92.6%). This was followed by deep superior sulcus deformity (n=125, 70.6%), ptosis (n=95, 53.6%), fornix shortening (n=93, 52.5%), volume deficiency (n=55, 31.1%), conjunctival papillae (n=54, 30.5%), pyogenic granulomas (n=43, 24.2%), wound dehiscence (n=42, 23.7%), and implant extrusion (n=30, 16.9%). Mild socket contraction was frequently reported in both countries, referred to by 79 ophthalmologists in Brazil (69.9%) and 49 in Spain (76.6%) (p<0.001). However, severe contraction with pronounced fornix shortening was more frequently observed in Brazil (n=22, 19.4%) (Table 2). Common complications with the EOP itself included surface deposits (n=70, 39.5%), scratches (n=62, 35%), and poor hygiene (n=54, 30.5%), finding statistically significant differences between the two groups (p<0.001) (Table 2).
External ocular prosthesis management
EOP management practices varied between the two countries. In Brazil, the majority of surgeons recommended either daily (n=53, 46.9%) or weekly (n=41, 36.2%) cleaning of the prosthesis. However, most Spanish surgeons advised monthly cleaning (n=31, 48.4%), a difference that was statistically significant (p<0.001) (Table 3). Additionally, a significant proportion of Brazilian surgeons (n=83, 73.4%) advised patients to remove the prosthesis before sleeping, whereas only a small minority of Spanish surgeons (n=3, 4.6%) recommended this practice (p<0.001) (Table 3).
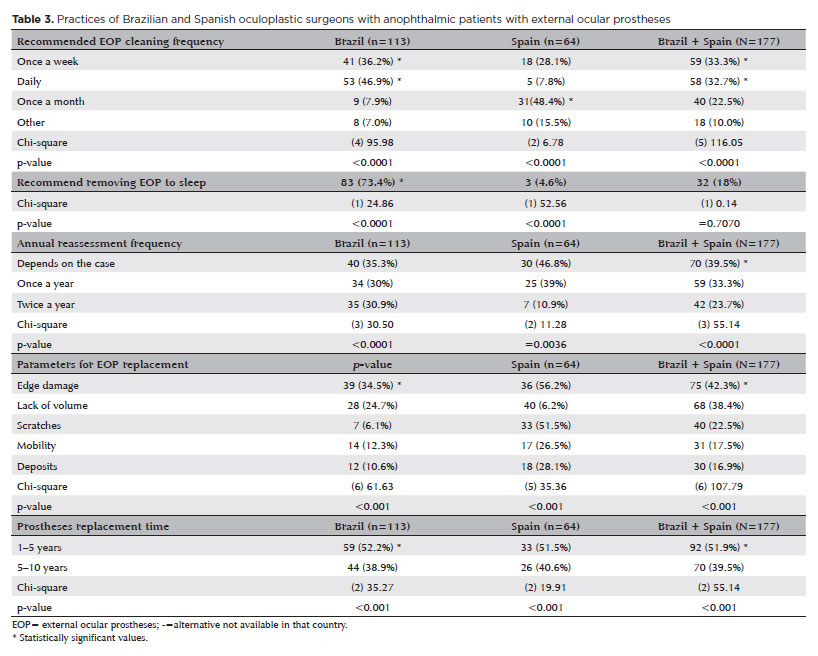
Follow-up frequencies reported for patients with EOPs varied. While 70 respondents (39.5%) indicated that reassessment intervals depended on the individual case, 59 (33.3%) recommended annual follow-ups (p<0.001) (Table 3).
The primary criteria for recommending EOP replacement included edge damage (75; 42.3%), loss of volume (68; 38.4%), and the presence of scratches (40; 22.5%). The most commonly reported replacement interval was every 1–5 years (92; 51.9%) (p<0.001) (Table 3).
DISCUSSION
This study examined the management of anophthalmic sockets by oculoplastic surgeons from two continents, revealing diverse approaches to clinical care. Given the limited literature on this subject and the absence of standardized treatment protocols, our findings contribute valuable insights into this underexplored topic(1,2).
A greater number of responses were obtained from Brazil, likely reflecting the greater number of practicing oculoplastic surgeons there. The overall response rate was 25%, lower than that obtained in previous studies (33.7%(3); 46%(6); 58%(7)), yet adequate for a reasonable sample size.
The majority of respondents had graduated within the last two decades, suggesting that they possessed substantial clinical experience in managing anophthalmic sockets and EOPs. Consistent with the findings of a previous study(8), the most commonly reported indication for eye removal was a blind, painful eye. This is the terminal manifestation of various ocular pathologies and a leading cause of acquired anophthalmia(9).
Among all of the respondents, evisceration was the preferred surgical technique over enucleation. This is in line with the current global preference for evisceration in non-tumoral cases due to its lesser surgical trauma and superior aesthetic outcomes(8,10).
Orbital implant material preferences among oculoplastic surgeons have evolved over time in parallel with technological advances. In the United States, hydroxyapatite was the standard in the early 1990s(11). However, by 2002, PP had become the material of choice(12). Similarly, UK surgeons surveyed in 2004 were found to predominantly use PP(13). In the present study, Brazilian surgeons preferred polymethyl methacrylate (PMMA) implants, corroborating the results of a national survey conducted in 2012(14). This preference may be driven by cost considerations, as PMMA is more affordable and orbital implants are not reimbursed by the Brazilian public health system. In contrast, surgeons in Spain, where implants are funded by the public health service, predominantly used PP implants. This was also consistent with previous findings(15). Most respondents favored spherical orbital implants, which are the most widely used implant shape internationally(14,16).
As documented in previous studies(17-20), our respondents reported a high incidence of discharge in anophthalmic sockets. While discharge may signal conjunctival inflammation, it can be exacerbated by scratches or deposits on the surface of the EOP or inadequate hygiene(21). Additional contributing factors can include tear film abnormalities, impaired lacrimal drainage, and eyelid dysfunction.
Clinical signs such as deep superior sulcus, ptosis, and socket contraction were prevalent, even after adequate rehabilitation. These often reflect orbital volume deficiency(22). Despite optimal implant sizing, factors such as the positioning, shape, and volume of the EOP can affect the contour of the superior sulcus(12,23). Deep superior sulcus and ptosis are also characteristic of anophthalmic socket syndrome(24), which results from the posterior displacement of orbital tissue following enucleation or evisceration(25). Even with careful implant placement, the levator palpebrae superioris and superior rectus muscles may shift toward the orbital apex, creating a volume void in the superior orbit(25).
Ptosis can also arise from repeated eyelid manipulation during EOP insertion and removal. This can lead to levator aponeurosis dehiscence, a phenomenon analogous to ptosis caused by long-term contact lens use, chronic eye rubbing, and floppy eyelid syndrome(26,27). Rather than tissue elongation, altered positioning appears to be the underlying cause. In predisposed individuals, prolonged EOP wear may contribute to this phenomenon. Adjustments in EOP design can improve eyelid height, but this can sometimes induce lagophthalmos(27).
Progressive fornix shortening is a recognized sequela of long-term prosthetic use(28). It is likely due to repeated mechanical trauma to the conjunctiva. Mild fornix shortening was most frequently reported by our respondents, over severe fornix shortening and no contraction. Successful rehabilitation requires adequate fornix depth to ensure prosthesis retention and satisfactory cosmetic outcomes. Inadequate depth can significantly affect a patient’s appearance and psychosocial well-being(29).
EOP maintenance practices varied widely among surgeons. Consistent with prior local data(2), daily cleaning and nighttime removal were most commonly recommended in Brazil. In contrast, most Spanish surgeons advised monthly cleaning and continuous wear, consistent with other international reports(30). Higher blinking frequency has been linked to increased discharge and prosthesis removal, prompting Spanish clinicians to advise against daily removal(19,23).
In both countries, follow-up frequency was typically individualized. Chronic EOP use, particularly with older prostheses, is associated with discharge, surface scratching, and poor hygiene, which can lead to biofilm formation and chronic inflammation. These conditions can, in turn, cause giant papillary conjunctivitis, a common complication in anophthalmic sockets(17).
Most respondents recommended replacing EOPs every 1–5 years, particularly when edge damage was present. Proper prosthesis care, including annual cleaning and polishing, can extend the lifespan of an EOP by preserving surface smoothness and wettability, thereby minimizing conjunctival irritation when blinking(17,19). Cleaning can be performed manually using water or mild surfactants, followed by air drying. The use of tissues or towels is discouraged due to the risk of surface scratches and microbial contamination(1,3,31,32).
Web-based surveys offer a practical means of collecting data from a larger number of geographically dispersed participants(6). However, this study had some limitations. Most notable among these was its reliance on self-reported practices from surgeons who responded voluntarily. Self-reported questionnaire responses can be less reliable than more objective means of data collection, while samples comprised only of respondents who chose to participate may not be generalizable to all practitioners in the given country. Interpretations should be based on the most commonly reported practices. However, this may inadvertently suggest that less frequently used approaches are inferior, which may not necessarily be the case.
Nonetheless, given the lack of standardized guidelines for the clinical management of anophthalmic sockets, this study provides important insights. The perspectives of Brazilian and Spanish oculoplastic surgeons regarding implant selection, clinical challenges, and EOP care may serve as a valuable reference for other practitioners, enhancing patient outcomes in this unique population.
In conclusion, while oculoplastic surgeons in Brazil and Spain largely employ comparable approaches to the management of anophthalmic sockets, differences were found in the types of implants used, the recommended frequency of prosthesis cleaning, and the recommendations given regarding the removal of EOPs before sleeping.
ACKNOWLEDGEMENTS
We would like to acknowledge all participants in our survey.
AUTHOR CONTRIBUTIONS:
Significant contribution to conception and design: Alicia Galindo-Ferreiro, Silvana Artioli Schellini. Data acquisition: Elvira Martinez-Fernandez, Carolina Pereira Bigheti. Data analysis and interpretation: Elvira Martinez-Fernandez, Carolina Pereira Bigheti. Manuscript drafting: Alicia Galindo-Ferreiro, Elvira Martinez-Fernandez, Carolina Pereira Bigheti. Significant intellectual content revision of the manuscript: Alicia Galindo-Ferreiro, Silvana Artioli Schellini. Final approval of the submitted manuscript: Alicia Galindo-Ferreiro, Elvira Martinez-Fernandez, Carolina Pereira Bigheti, Denisse Casia Morerira Zornoff, Hortensia Sanchez-Tocino, Silvana Artioli Schellini. Statistical analysis: Denisse Casia Morerira Zornoff, Hortensia Sanchez-Tocino. Obtaining funding: not applicable. Supervision of administrative, technical, or material support: Alicia Galindo-Ferreiro, Silvana Artioli Schellini. Research group leadership: Alicia Galindo-Ferreiro, Silvana Artioli Schellini.
REFERENCES
1. Bonaque-González S, Amigó A, Rodríguez-Luna C. Recommendations for post-adaption care of an ocular prosthesis: A review. Cont Lens Anterior Eye. 2015;38(6):397-401.
2. Martinez-Fernandez E, Pereira Bigheti C, Sanchez-Tocino H, Moreira Zornoff D, Schellini SA, Galindo-Ferreiro A. Management of external ocular prosthesis by ocularists: results of an online survey conducted in Brazil and Spain. Int Ophthalmol. 2023;43(11):4297-304.
3. Osborn KL, Hettler D. A survey of recommendations on the care of ocular prostheses. Optometry. 2010;81(3):142-5.
4. Questionnaire directed to ophthalmologists abour anophthalmic sockets, in Portuguese - REDCap [Internet]. 2021. [cited 19/07/2025]. Available from: https://redcap.hcfmb.unesp.br/ surveys/?s=J9Y37EY74L
5. Questionnaire directed to ophthalmologists abour anophthalmic sockets, in Spanish - REDCap [Internet]. 2021. [cited 19/07/2025]. Available from: https://redcap.hcfmb.unesp.br/surveys/?s=NKJAMNMDFK
6. Chinnery H, Thompson SBN, Noroozi S, Dyer B, Rees K. Questionnaire study to gain an insight into the manufacturing and fitting process of artificial eyes in children: an ocularist perspective. Int Ophthalmol. 2017;37(5):1175-83.
7. Hintschich C, Baldeschi L. Rehabilitation of anophthalmic patients. Results of a survey. Ophthalmologe. 2001;98(1):74-80.
8. Al-Dahmash SA, Bakry SS, Almadhi NH, Alashgar LM. Indications for enucleation and evisceration in a tertiary eye hospital in Riyadh over a 10-year period. Ann Saudi Med. 2017;37(4):313-6.
9. Vardizer Y, Sobeh T, Prat DL, Ben Simon GJ, Tomkins-Netzer O. Assessing the results of anophthalmic prostheses. Indian J Ophthalmol. 2021;69(7):1876-81.
10. Quaranta-Leoni FM, Fiorino MG, Quaranta-Leoni F, Di Marino M. Anophthalmic Socket Syndrome: Prevalence, Impact and Management Strategies. Clin Ophthalmol. 2021;15:3267-81.
11. Hornblass A, Biesman BS, Eviatar JA. Current techniques of enucleation: a survey of 5,439 intraorbital implants and a review of the literature. Ophthalmic Plast Reconstr Surg. 1995;11(2):77-8.
12. Su GW, Yen MT. Current trends in managing the anophthalmic socket after primary enucleation and evisceration. Ophthalmic Plast Reconstr Surg. 2004;20(4):274-80.
13. Viswanathan P, Sagoo MS, Olver JM. UK national survey of enucleation, evisceration and orbital implant trends. Br J Ophthalmol. 2007;91(5):616-9.
14. Sousa RLF de, Schellini SA, Zornoff D de CM, Padovani CR. Trends on anophthalmic socket repair in Brazil. Arq Bras Oftalmol. 2012;75(6):394-7.
15. Alwitry A, West S, King J, Foss AJ, Abercrombie LC. Long-term follow-up of porous polyethylene spherical implants after enucleation and evisceration. Ophthalmic Plast Reconstr Surg. 2007;23(1):11-5.
16. Schellini SA. Perspectives on the clinical feasibility of techniques used in anophthalmic socket reconstruction. Exp Rev Ophthalmol. 2023;18(4):227-30.
17. Pine KR, Sloan BH, Jacobs RJ. A proposed model of the response of the anophthalmic socket to prosthetic eye wear and its application to the management of mucoid discharge. Med Hypotheses. 2013;81(2):300-5.
18. Pine K, Sloan B, Stewart J, Jacobs RJ. Concerns of anophthalmic patients wearing artificial eyes. Clin Exp Ophthalmol. 2011;39(1):47-52.
19. Kashkouli MB, Zolfaghari R, Es’haghi A, Amirsardari A, Abtahi MB, Karimi N, et al. Tear film, lacrimal drainage system, and eyelid findings in subjects with anophthalmic socket discharge. Am J Ophthalmol. 2016;165:33-8.
20. Pine NS, de Terte I, Pine KR. An investigation into discharge, visual perception, and appearance concerns of prosthetic eye wearers. Orbit (London). 2017;36(6):401-6.
21. Chang WJ, Tse DT, Rosa RH, Huang A, Johnson TE, Schiffman J. Conjunctival cytology features of giant papillary conjunctivitis associated with ocular prostheses. Ophthalmic Plast Reconstr Surg. 2005;21(1):39-45.
22. Ruiters S, Mombaerts I. The prevalence of anophthalmic socket syndrome and its relation to patient quality of life. Eye (Lond). 2020;35(7):1909-14.
23. Kaltreider SA, Shields MD, Hippeard SC, Patrie J. Anophthalmic ptosis: investigation of the mechanisms and statistical analysis. Ophthalmic Plast Reconstr Surg. 2003;19(6):421-8.
24. Choi B hun, Lee S hyeok, Chung W sun. Correction of superior sulcus deformity and enophthalmos with porous high-density polyethylene sheet in anophthalmic patients. Korean J Ophthalmol. 2005;19(3):168-73.
25. Smit TJ, Koornneef L, Zonneveld FW, Groet E, Otto AJ. Primary and secondary implants in the anophthalmic orbit: preoperative and postoperative computed tomographic appearance. Ophthalmology. 1991;98(1):106-10.
26. Van den Bosch WA, Lemij HG. Blepharoptosis induced by prolonged hard contact lens wear. Ophthalmology. 1992;99(12): 1759-65.
27. Mombaerts I, Groet E. Upper eyelid ptosis surgery using a preparatory ocular prosthesis. Ophthalmic Plast Reconstr Surg. 2009;25(2):90-3.
28. Jones DF, Lyle CE, Fleming JC. Superior conjunctivoplasty-mullerectomy for correction of chronic discharge and concurrent ptosis in the anophthalmic socket with enlarged superior fornix. Ophthalmic Plast Reconstr Surg. 2010;26(3):172-5.
29. Nabavi CB, Long JA, Compton CJ, Vicinanzo MG. A novel surgical technique for the treatment of giant fornix syndrome. Ophthalmic Plast Reconstr Surg. 2013;29(1):63-6.
30. Pine KR, Sloan B, Stewart J, Jacobs RJ. The response of the anophthalmic socket to prosthetic eye wear. Clin Exp Optom. 2013;96(4):388-93.
31. Toribio A, Marrodán T, Fernández-Natal I, Martínez-Blanco H, Rodríguez-Aparicio L, Ferrero M. Study of conjunctival flora in anophthalmic patients: influence on the comfort of the socket . Graefes Arch Clin Exp Ophthalmol. 2017;255(8):1669-79.
32. Baino F, Potestio I. Orbital implants: State-of-the-art review with emphasis on biomaterials and recent advances. Mater Sci Eng C Mater Biol Appl. 2016;69:1410-28.
Submitted for publication:
February 28, 2025.
Accepted for publication:
June 5, 2025.
Approved by the following research ethics committee: Faculdade de Medicina de Botucatu – UNESP (CAAE: 61568816.3.0000.5411).
Data Availability Statement: The contents underlying the research text are included in the manuscript
Edited by
Editor-in-Chief: Newton Kara-Júnior
Associate Editor: Fernando Procianoy
Funding: This study received no specific financial support.
Disclosure of potential conflicts of interest: The authors declare no potential conflicts of interest.

How to cite this article:
 ABO is licensed under a Creative Commons Attribution-NonComercial 4.0 Internacional.
ABO is licensed under a Creative Commons Attribution-NonComercial 4.0 Internacional.