Arq. Bras. Oftalmol. 2026; 89 (4): 10.5935/0004-2749.2025-0344
Total: 26
Mehmet Özbaş; Bengi Demirayak
DOI: 10.5935/0004-2749.2025-0344
ABSTRACT
PURPOSE: This study aimed to evaluate early postoperative changes in retinal microvasculature in patients undergoing cardiopulmonary bypass surgery by comparing preoperative and postoperative measurements of superficial capillary plexus and, deep capillary plexus vessel density, foveal avascular zone area using optical coherence tomography angiography (OCT-A).
METHODS: This prospective longitudinal study included 38 patients, undergoing cardiopulmonary bypass surgery. Each patient served as their own control optical coherence tomography angiography imaging was performed at four time points: 3 days preoperatively and at postoperative week 1, week 2, and month 1. Vessel densities in the superficial capillary plexus and deep capillary plexuses and the foveal avascular zone area were measured and analyzed. Depending on data distribution repeated measures analysis of variance or the Friedman test was used for statistical analysis.
RESULTS: Data from all 38 patients were included in the analysis. A significant increase in overall superficial capillary plexus vessel density was observed following cardiopulmonary bypass surgery (p=0.008). In contrast, deep capillary plexus vessel density did not differ significantly between the preoperative and postoperative assessments. The foveal avascular zone area showed a significant increase at postoperative week 2 compared with baseline (p=0.016).
CONCLUSION: Cardiopulmonary bypass surgery may induce early retinal microvascular alterations, particularly in the superficial capillary plexus and foveal avascular zone. Optical coherence tomography angiography is a noninvasive and reproducible imaging modality that enables precise assessment of subtle retinal vascular changes after major cardiovascular surgery. These findings may contribute to postoperative monitoring and risk assessment in patients undergoing cardiopulmonary bypass.
Keywords: Cardiopulmonary bypass surgery; Extracorporeal circulation; Macular vessel density of the retina; Retina/blood supply; Foveal avascular zone; Optical coherence tomography angiography; Retinal microvasculature
INTRODUCTION
Cardiopulmonary bypass (CPB) is a life-saving technique widely used during complex cardiac surgeries to maintain systemic circulation and oxygenation through an extracorporeal circulation system(1,2). Despite its clinical benefits, CPB is associated with severe systemic complications, including microvascular alterations that may affect multiple organs, including the retina(2-4).
Postoperative visual loss is a rare but potentially devastating complication of CPB, with reported incidences ranging from 0.06% to 0.33%(5-7). Several mechanisms have been proposed to explain this complication, including hemodynamic and hematologic disturbances, embolic events, ischemic optic neuropathy, retinal nerve fiber damage, chorioretinal hypoperfusion, and tissue hypoxia. These factors may contribute to retinal ischemia and subsequent visual dysfunction(8).
Although systemic hypoperfusion and hypotension frequently occur during CPB, their effects on macular perfusion remain poorly understood. Optical coherence tomography angiography (OCT-A) is a non-invasive, high-resolution imaging technique that enables visualization and quantitative assessment of retinal and choroidal microvasculature(9).
A better unterstandig of early retinal microvascular alterations after CPB may help identify patients at risk of ocular complications and inform postoperative surveillance strategies. Therefore, this study aimed to evaluate retinal microvascular changes following CPB surgery by comparing OCT-A parameters obtained preoperatively with those measured at postoperative week 1, week 2, and month 1.
METHODS
This prospective longitudinal observational study was conducted at the Department of Ophthalmology, University of Health Sciences Bakırköy Dr. Sadi Konuk Training and Research Hospital, Istanbul, Turkey, in accordance with the principles of the Declaration of Helsinki. Written informed consent was obtained from all participants before enrollment. The study protocol was approved by the local institutional ethics committee.
Between March and December 2023, patients scheduled to undergo CPB surgery for coronary artery bypass grafting (CABG) at the Department of Cardiovascular Surgery were referred to the Department of Ophthalmology for preoperative evaluation. Patients with systemic diseases other than well-controlled hypertension and hyperlipidemia were excluded. Additional exclusion criteria included a history of intraocular surgery, orbital trauma, ocular disorders that could affect OCT-A image quality (e.g., advanced cataract, corneal opacity, or vitreous hemorrhage), and hypertensive retinopathy.
All patients underwent CPB using a cardiopulmonary bypass system equipped with a hollow-fiber membrane oxygenator and a 40-μm arterial filter. During aortic cross-clamping, pulsatile flow was maintained at 2.4 L/min/m2. After removal of the cross-clamp, continuous flow was established. Systemic hypothermia was induced and maintained at 29°C-30°C, and mean arterial pressure was maintained between 50 and 60 mmHg throughout the procedure. Myocardial protection was achieved using intermittent antegrade cold blood cardioplegia with a blood-to-crystalloid ratio of 4:1(10).
A total of 38 eyes from 38 patients were included in the analysis. All participants underwent a comprehensive ophthalmologic examination before surgery, including best-corrected visual acuity (BCVA) assessment, slit-lamp biomicroscopy, and dilated fundus examination. BCVA assessment and OCT-A imaging were repeated at postoperative weeks 1 and 2 and at month 1. Demographic and perioperative data were collected for all participants.
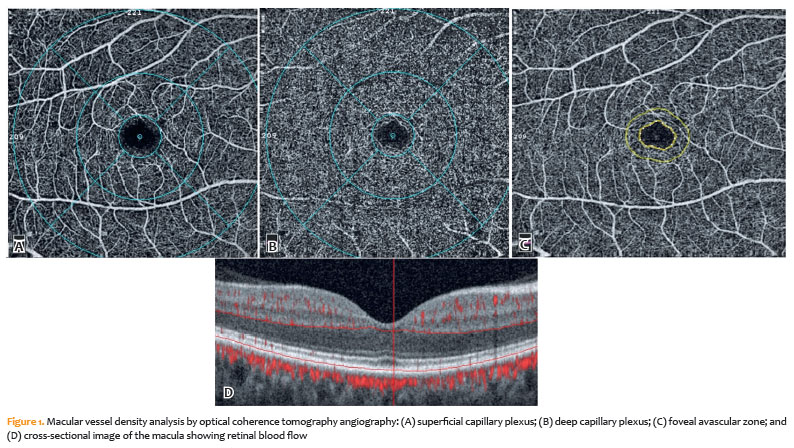
OCT-A imaging was performed using a split-spectrum amplitude-decorrelation angiography algorithm implemented in the RTVue XR Avanti system with AngioVue software (Optovue Inc., Fremont, California). For each participant, 6×6-mm macular scans were obtained. Automated layer segmentation was used to identify the superficial capillary plexus (SCP) and deep capillary plexus (DCP).
Vessel density (VD, %) measurements were recorded for the whole image, as well as the foveal, parafoveal, and perifoveal regions. Regional analyses were further performed in the superior, nasal, inferior, and temporal quadrants. The foveal avascular zone (FAZ) area was measured in square millimeters (mm2). Representative OCT-A images of the SCP, DCP, and FAZ are presented in figure 1.
All OCT-A images underwent quality assessment before analysis. Scans with a signal strength index <6, segmentation errors, or significant motion artifacts were excluded. Two independent graders evaluated all images, and any discrepancies were resolved through consensus.
Statistical analysis
Statistical analyses were performed using IBM SPSS Statistics for Windows, version 26.0 (IBM Corp., Armonk, New York). Continuous variables are presented as mean ± standard deviation (SD), with minimum and maximum values where appropriate.
The distribution of quantitative variables was assessed using the Kolmogorov-Smirnov test, Shapiro-Wilk test, skewness and kurtosis values, and graphical methods, including histograms and quantile-quantile (Q-Q) plots.
Because measurements were obtained repeatedly at four time points, variables with a normal distribution were analyzed using repeated measures analysis of variance (ANOVA). In contrast, nonnormally distributed variables were analyzed using the Friedman test. When significant overall differences were identified, post hoc pairwise comparisons were performed. For normally distributed variables, paired t tests with adjustment for multiple comparisons were used. For nonnormally distributed variables, Wilcoxon signed-rank tests with appropriate correction for multiple testing were applied.
All statistical tests were two-sided, and a p value <0.05 was considered statistically significant.
RESULTS
A total of 38 eyes from 38 patients were included in the final analysis. Of the 47 patients initially enrolled, two were excluded because of postoperative mortality, one because of diabetic retinopathy, and six because of inadequate OCT-A image quality.
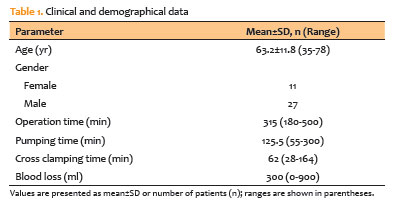
The study population comprised 11 women (28.9%) and 27 men (71.1%), with a mean age of 63.2±11.8 yr (range, 35-78 yr). The demographic and clinical characteristics of the participants are summarized in table 1.
Measurements of vessel density (VD) in the SCP and DCP, including whole-image, foveal, parafoveal, and perifoveal parameters as well as FAZ area measurements are presented in table 2. Comparisons between preoperative and postoperative measurements are summarized in table 3.
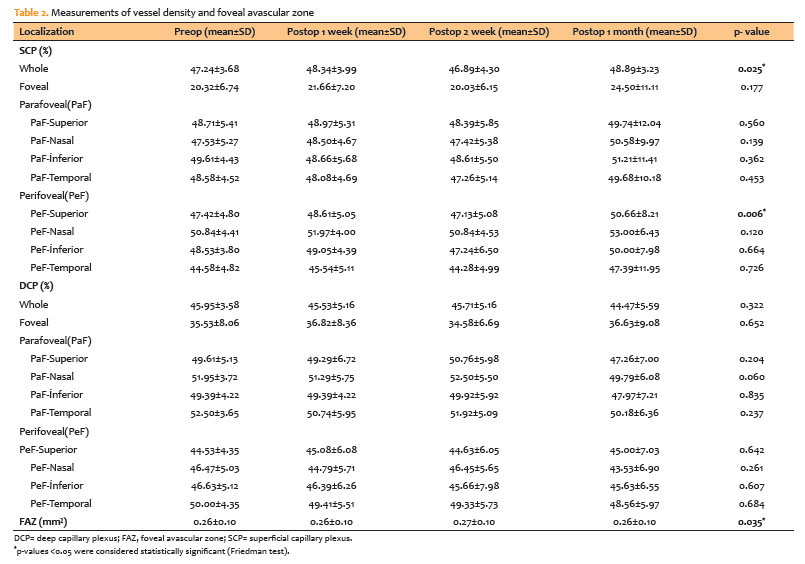
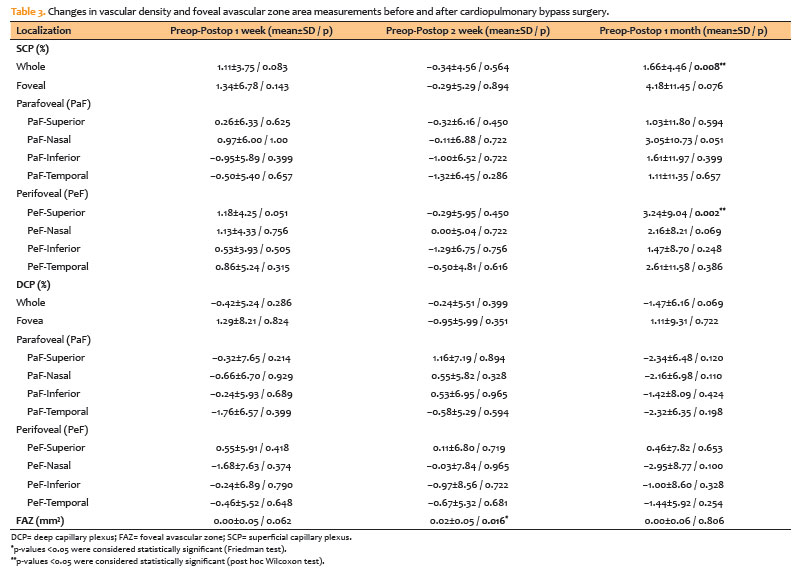
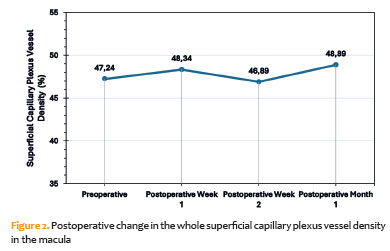
A significant increase in overall SCP vessel density was observed during the postoperative follow-up period. Mean SCP vessel density increased from 47.24% preoperatively to 48.89% at postoperative month 1 (p=0.008; Table 2). Changes in macular SCP vessel density over time are illustrated in Figure 2. In addition, SCP vessel density in the superior perifoveal region increased significantly at postoperative month 1 compared with baseline values (p=0.002; Table 3).
No significant differences were detected in DCP vessel density between the preoperative and postoperative assessments. In contrast, the FAZ area increased significantly at postoperative week 2 (p=0.016) and subsequently returned to values comparable to baseline by postoperative month 1 (Table 3).
Postoperative ophthalmologic examinations revealed no newly developed ocular abnormalities during the follow-up period. BCVA remained stable throughout the study and did not differ significantly from preoperative values.
DISCUSSION
Many studies have reported that blood flow in the optic nerve head (ONH) decreases during CPB, and ischemic optic neuropathy is one of the most common complications resulting from hypoperfusion(11,12). In addition, non-arteritic anterior ischemic optic neuropathy and posterior ischemic optic neuropathy may occur because of severe hypoperfusion caused by hypotension(12). However, it remains unclear whether macular perfusion is affected by the systemic hypoperfusion and hypotension associated with CPB. Only a few studies have investigated this issue. Therefore, in the present study, we aimed to evaluate macular microvascular changes in patients undergoing CPB surgery.
Fundus fluorescein angiography (FFA) is considered the gold standard for evaluating retinal perfusion. In a previous study, retinal microvascular damage was detected by FFA in five of nine patients after CPB surgery(13). However, FFA is an invasive procedure, and patient compliance may be limited during the early postoperative period. OCT-A is a noninvasive technique that enables high-resolution imaging and provides accurate, objective measurements of the retinal layers, optic disc, and choroid(14,15).
The findings of Wang et al.(16) suggest that retinal microvasculature reflects systemic vascular status, supporting the concept that OCT-A can detect microvascular alterations associated with cardiovascular disease. In their study, mean macular vessel density was significantly lower in patients with coronary heart disease than in healthy controls, indicating chronic microvascular impairment. In this context, our findings may reflect acute postoperative changes superimposed on an underlying systemic vascular condition.
In the present study, we found that SCP vessel density at the macular level increased significantly within 1 month after CPB surgery, whereas no significant changes were observed in DCP vessel density. In addition, the FAZ area showed a transient increase at postoperative week 2 and returned to baseline values by postoperative month 1. These findings suggest that CPB surgery may induce early alterations in superficial retinal perfusion, possibly reflecting autoregulatory responses to intraoperative hypotension.
Other mechanisms may also contribute to the increase in SCP vessel density. The inflammatory response associated with CPB may increase retinal vascular permeability and vasodilation. Furthermore, hemodilution and hypoxemia during surgery may temporarily increase vessel diameter in response to elevated tissue oxygen demand.
Similarly, Li et al.(17) reported improved retinal microcirculation after cardiac surgery. Our findings are generally consistent with this observation and may indicate increased retinal perfusion during the early postoperative period. This change may be related to compensatory vascular responses or restoration of systemic circulation following surgery.
The SCP consists of larger arterioles, capillaries, and venules and is closely associated with the central retinal artery, whereas the DCP is supplied through vertical anastomoses originating from the superficial plexus(18). According to our findings, the SCP appears to be more affected by systemic hemodynamic changes, whereas the DCP appears to be less susceptible to alterations in systemic circulation.
The structural organization of the DCP differs from that of the SCP. OCT-A studies have shown that the DCP is located in deeper retinal layers and exhibits a vortex-like capillary network pattern. The SCP is more directly connected to the central retinal arterial circulation, whereas the DCP is supplied through vertical interconnections from the superficial plexus(19,20).
These anatomical differences may contribute to variations in perfusion dynamics between retinal vascular layers and may explain their differential susceptibility to acute systemic hemodynamic changes. The observed increase in SCP vessel density may represent a compensatory response aimed at preserving perfusion in the deeper retinal layers.
Although direct evidence remains limited, the differential response observed between the SCP and DCP may be explained by their distinct anatomical organization and vascular connectivity.
The FAZ area measured 0.26 mm2 preoperatively, at postoperative week 1, and at postoperative month 1. However, it increased to 0.27 mm2 at postoperative week 2, and this difference was statistically significant compared with the preoperative value (p=0.035; Table 2). This transient enlargement of the FAZ area may be attributed to intraoperative hypotension and hypoperfusion during aortic cross-clamping in CPB surgery. The subsequent normalization of the FAZ area by postoperative month 1 may reflect improved perfusion or autoregulatory mechanisms within the retinal microcirculation.
In contrast, Simdivar et al.(21) did not observe significant changes in retinal vessel density or FAZ area after CPB surgery. Several methodological and clinical differences may explain this discrepancy. First, they used a 3 × 3-mm OCT-A scan protocol, which evaluates a more limited central macular area, whereas our study used 6 × 6 mm scans, allowing a more comprehensive assessment of the macular microvasculature. Second, their study population included patients with systemic comorbidities such as diabetes mellitus and chronic renal failure, both of which are known to affect microvascular structure and function. In contrast, our study population was relatively homogeneous because patients with systemic diseases other than well-controlled hypertension and hyperlipidemia were excluded. This may have minimized potential confounding effects on retinal microvasculature and facilitated the detection of subtle postoperative microvascular changes.
The relatively small sample size is the main limitation of this study. Although systemic vascular factors, including the severity and laterality of coronary artery occlusion and the presence of concomitant carotid artery disease, may influence retinal microcirculation, the primary objective of this study was to isolate the effect of CPB using a within-subject longitudinal design. Each patient served as their own control, allowing the assessment of longitudinal changes while minimizing interindividual variability. Therefore, factors such as the severity and laterality of coronary artery occlusion and concomitant carotid artery disease were beyond the scope of the present analysis.
In this study, we found that CPB surgery has an early effect on retinal microcirculation and may increase vessel density, particularly in the SCP. The preservation of DCP vessel density and the transient changes observed in the FAZ area suggest distinct physiological responses among retinal vascular layers. These microvascular alterations occurred without any change in visual acuity. In conclusion, CPB surgery may cause a subclinical increase in macular vessel density. Larger prospective studies are needed to confirm these findings and improve their generalizability.
ACKNOWLEDGMENTS
The authors sincerely acknowledge Emire Bor for her contribution to the statistical analyses and express their gratitude to the cardiovascular surgeons Saygın Türkyılmaz, Gülsüm Türkyılmaz, Filiz Bakkal, and Ali Aycan Kavala for their invaluable contributions to this study. They also thank Enago (www.enago.br) for the English language review.
AUTHORS' CONTRIBUTIONS:
Significant contribution to conception and design: Mehmet Özbaş.
Data Acquisition: Mehmet Özbaş.
Data Analysis and Interpretation: Mehmet Özbaş, Bengi Demirayak.
Manuscript Manuscript Drafting: Mehmet Özbaş.
Significant intellectual content revision of the manuscript: Mehmet Özbaş, Bengi Demirayak.
Final approval of the submitted manuscript: Mehmet Özbaş, Bengi Demirayak.
Statistical analysis: Mehmet Özbaş, Bengi Demirayak.
Obtaining funding: not applicable.
Supervision of administrative, technical, or material support: Mehmet Özbaş.
Research group leadership: Mehmet Özbaş.
REFERENCES
1. Singha SK, Karim HR, Panda CK. Cardiopulmonary bypass: basic principles and updates in anaesthetic management. ARC J Anesthesiol. 2018;3(2):14-20.
2. Roberts A, Duncan EC, Hargrave P, Kingery DR, Barnes J, Horstemeyer DL, et al. Complications of cardiopulmonary bypass from an anesthesia perspective: a clinical review. HCA Healthc J Med. 2023;4(1):13-21.
3. Raphael J, Moss HE, Roth S. Perioperative visual loss in cardiac surgery. J Cardiothorac Vasc Anesth. 2019;33(5):1420-9.
4. Fosnot J, Glazer-Hockstein C, Tolentino MJ. Central retinal vein occlusion immediately following cardiac surgery. Ophthalmic Surg Lasers Imaging. 2003;34(3):215-6.
5. Hayashi H, Kawaguchi M, Hasuwa K, Inoue S, Okamoto M, Matsuura T, et al. Changes in intraocular pressure during cardiac surgery with and without cardiopulmonary bypass. J Anesth. 2010;24(5):663-8.
6. Nuttall GA, Garrity JA, Dearani JA, Abel MD, Schroeder DR, Mullany CJ. Risk factors for ischemic optic neuropathy after cardiopulmonary bypass: A matched case/control study. Anesth Analg. 2001;93(6):1410-6.
7. Sweeney PJ, Breuer AC, Selhorst JB, Waybright EA, Furlan AJ, Lederman RJ, et al. Ischemic optic neuropathy: a complication of cardiopulmonary bypass surgery. Neurology. 1982;32(5):560-2.
8. Nenekidis I, Pournaras CJ, Tsironi E, Tsilimingas N. Vision impairment during cardiac surgery and extracorporeal circulation: current understanding and the need for further investigation. Acta Ophthalmol. 2012;90(3):e168-72.
9. Tan AC, Tan GS, Denniston AK, Keane PA, Ang M, Milea D, et al. An overview of the clinical applications of optical coherence tomography angiography. Eye (Lond). 2018;32(2):262-86.
10. Stoney WS. Evolution of cardiopulmonary bypass. Circulation. 2009;119(21): 2844-53.
11. Nenekidis I, Geiser M, Riva C, Pournaras C, Tsironi E, Vretzakis G, et al. Blood flow measurements within optic nerve head during on-pump cardiovascular operations. A window to the brain? Interact Cardiovasc Thorac Surg. 2011;12(5):718-22. Comment in: Interact Cardiovasc Thorac Surg. 2011; 12(5):722;discussion 722-3.
12. Hayreh SS. Ischemic optic neuropathy. Prog Retin Eye Res. 2009;28(1):34-62.
13. Ascione R, Ghosh A, Reeves BC, Arnold J, Potts M, Shah A, et al. Retinal and cerebral microembolization during coronary artery bypass surgery: a randomized controlled trial. Circulation. 2005;112(25):3833-8. Comment in: Circulation. 2005;112(25):3816-7.
14. de Carlo TE, Romano A, Waheed NK, Duker JS. A review of optical coherence tomography angiography (OCTA). Int J Retina Vitreus. 2015;1:5.
15. Al- Sheikh M, Tepelus TC, Nazikyan T, Sadda SR. Repeatability of automated vessel density measurements using optical coherence tomography angiography. Br J Ophthalmol. 2017;101(4):449-52.
16. Wang J, Jiang J, Zhang Y, Qian YW, Zhang JF, Wang ZL. Retinal and choroidal vascular changes in coronary heart disease: an optical coherence tomography angiography study. Biomed Opt Express. 2019;10(4):1532-44.
17. Li C, Zhu Z, Yuan H, Zhong P, Peng Q, Dong X, et al. Improved retinal microcirculation after cardiac surgery in patients with congenital heart disease. Front Cardiovasc Med. 2021;8:712308.
18. Provis JM. Development of the primate retinal vasculature. Prog Retin Eye Res. 2001;20(6):799-821.
19. Bonnin S, Mané V, Couturier A, Julien M, Paques M, Tadayoni R, et al. New ınsıght ınto the macular deep vascular plexus ımaged by optıcal coherence tomography angıography. Retina. 2015;35(11):2347-52.
20. Hormel TT, Jia Y, Jian Y, Hwang TS, Bailey ST, Pennesi ME, et al. Plexus-specific retinal vascular anatomy and pathologies as seen by projection-resolved optical coherence tomographic angiography. Prog Retin Eye Res. 2021;80:100878.
21. Simdivar GH, Incekalan TK, Gunduz A. Evaluation of retinal and peripapillary vessel density and subfoveal choroidal thickness changes in patients undergoing cardiopulmonary bypass: An OCTA study. Indian J Ophthalmol. 2024; 72(Suppl 1):119-24.
Submitted for publication:
December 18, 2025.
Accepted for publication:
May 15, 2026.
Approved by the following research ethics committee: Bakırköy Dr. Sadi Konuk Training and Research Hospital (Approval No. 2025-04-09).
Data Availability Statement: The datasets produced and/or analyzed in this study can be provided to referees upon request.
Edited by
Editor-in-Chief: Newton Kara-Júnior
Associate Editor: Rodrigo P. C. Lira
Funding: This study received no specific financial support.
Disclosure of potential conflicts of interest: The authors declare no potential conflicts of interest.

How to cite this article:
 ABO is licensed under a Creative Commons Attribution-NonComercial 4.0 Internacional.
ABO is licensed under a Creative Commons Attribution-NonComercial 4.0 Internacional.